

Introduction
Funding long-term care (LTC) has been recognized as a huge issue for our country for a long time. Insurers, regulators, politicians, providers, educators and policy wonks continue to seek solutions.
For the purposes of this article, let’s assume that a client age 55 buys a Partnership-qualified policy with an initial monthly maximum of $4500, 3% compounding and a 3-year benefit period after a 90-service-day elimination period. Let’s assume the client begins to need qualifying care at age 85½, at which time her maximum monthly benefit would have risen to $11,044. For convenience, I’ll assume the insured/claimant is female and her life partner (if any) is male. If she uses the full amount each month, her LTCi benefits would be as follows:
| Insurance Age at the Beginning of the Claim Year | Maximum Monthly Benefit | Number of Months of Benefits Paid | Reimbursement of that Year’s Expenses | Comment |
| 85 | $11,044 | 3 | $33,132 | Claim started at mid-year; 90-day EP; so only 3 months paid |
| 86 | $11,375 | 12 | $136,500 | |
| 87 | $11,717 | 12 | $140,592 | |
| 88 | $12,068 | 9 | $108,612 | |
| Total | $418,836 |
The government benefits from that purchase of private LTCi in the following ways:
- The private insurance LTCi benefit of $418,836 likely kept the client off Medicaid or contributed to the cost of Medicaid care, saving money for both the Federal government and state government.
- For those kept off Medicaid, the state avoids the administrative cost of determining whether the insured is eligible for Medicaid, setting up records, and making payments.
- The state and Federal governments benefit because LTC providers get the full private pay rate rather than the reduced Medicaid rate. Providers are therefore better able to provide outstanding service. The more LTCi there is, the more likely it is that innovators will want to be in the LTC industry, providing new and better services.
- The additional revenue enables the provider to earn more profit and/or pay higher salaries. Thus, the provider and/or its employees pay higher income taxes to the state and Federal governments.
- With LTCi, the client is likely to be less dependent on family care. Thus, family members are likely to be more productive for society and to generate more income, which results in more income taxes for state and Federal governments.
- The insurance agent who sold LTCi will pay income taxes on his/her commissions to the state and Federal governments.
- The insurance company will pay premium tax to the state and income tax to the Federal government.
As noted in the above bullets, the insured person benefits, the insured’s family benefits, the providers and their employees benefit, insurance brokers and their families benefit, and insurers (and their employees and shareholders) benefit, as well as the state and Federal government.
The Robert Woods Johnson Foundation (Mark Meiners, in particular) brainstormed to find a way to protect the government from the LTC costs of an aging population. What could the government do to encourage the middle class to buy more LTCi? They developed a win-win-win-win-win-win concept to make private long-term care insurance (LTCi) more affordable for the middle class: State/Carriers Public Partnerships. In a nutshell, State Partnerships are an additional back-end safety net to reward middle-class people for buying LTCi.
Four states (CA, CT, IN and NY) blazed the trail for Partnership programs in the early 1990s. However, an aide to Congressman Henry Waxman incorrectly concluded that the Partnership was a boondoggle for the rich. So, Waxman inserted into Federal legislation (OBRA, 1993) a provision prohibiting other states from developing future Partnerships. The four existing programs (including his state, CA) were grandfathered.
Twelve years later, the Deficit Reduction Act of 2005 (DRA) removed the restriction, allowing more jurisdictions to create Partnership programs. Now, 45 states have Partnership programs. (Partnership policies are not available in AK, HI, MA, MS, or VT, nor in DC, Puerto Rico or Guam. However, MA has a similar program called MassHealth Exemption.) The original, grandfathered states’ provisions differ among themselves and also differ from the provisions of the other 41 “DRA” states. There are also slight differences among the DRA states, most particularly relative to what types of compound benefit provisions can qualify for Partnership status.
Medicaid Eligibility in General
When our claimant applies to Medicaid for long-term care services, state reviewers determine whether she is eligible for Medicaid (“Medi-Cal” in California) LTC benefits. The numbers in this section of the article apply in 2025, unless otherwise indicated.
- Any of her income in excess of $50/month (varies by state and may differ for home care) must be applied to the cost of care. If that income is sufficient to cover her entire cost of care, she is not eligible for Medicaid. Notes:
- Her spouse is entitled to his independent income (however, if he owns an annuity in payout mode that has a certain period or death benefit, the state must be identified as a secondary beneficiary.
- If her spouse is impoverished, she can transfer income to him to bring his income up to $2,555/month. He can appeal to get as much as $3,948/month, so some jurisdictions (AK, CA, DC, GA, IL, IA, LA, MS, NV, NY, OK, SC, TX, WY) automatically permit up to $3,948 instead of $2,555.
- Some states have an “income cap” ($2,901/month) rather than determining whether the income is sufficient to cover the cost of care. That is, if your income exceeds $2,901/month, you are ineligible for Medicaid LTC support. People who can’t afford their LTC but who earn too much income can put excess income into a Miller Trust which pays their provider. That brings their income within limits, qualifying them for Medicaid if they and their trust were unable to pay the full cost..
- In jurisdictions other than California, the care-needy individual must also apply “countable assets” in excess of $2,000 (in most states) toward the cost of care.
- Non-countable assets include:
- The person’s home (unless equity exceeds the amount shown below) if any of the following circumstances apply
- The person may return to the home
- The person’s spouse is living in the home
- The person’s child under age 21 or blind or permanently & totally disabled is living in the home
- A sibling is living in the home and resided in it for at least one year (while having an ownership interest) immediately before the person was admitted to the facility.
- A child is living in the home and resided in home for at least two years immediately before the person’s admission and provided care which permitted the person to stay home rather than be in an institution.
- The person is ineligible for Medicaid if home equity exceeds $730,000, except that the cap is $1,097,000 in CO, CT, DC, HI, MA, NJ, NY, and WA. (CA does not impose this limitation.) These limits are indexed each year.
- One automobile
- Household and personal belongings
- Wedding and engagement rings
- Income-generating property (because the income must be used to pay for care)
- Burial plot and prepaid burial plans
- Cash value of life insurance if, and only if, the combined death benefit under such policies is less than 1500.
- Term insurance
- The person’s home (unless equity exceeds the amount shown below) if any of the following circumstances apply
- To be clear “countable assets” include:
- Cash above the limit ($2000 or so for single people; $3000 or so for a couple who both need care)
- Other liquid assets: CDs, T-bills, stocks, bonds, retirement accounts (Keough*, 4.01k*, IRA*, 4.03b, etc.). Kansas is an exception in that the spouse’s §4.03B funds are exempt.
- Cash Value of life insurance if the combined death benefits exceeds $1500
- Vacation home
- Second vehicles
- Non-countable assets include:
Medicaid Repayment
Federal legislation (Public Law 104-191) requires that Medicaid costs be reimbursed by the recipient’s estate (“estate recovery”). When someone begins to need Medicaid support for LTC, the state may place a lien on that person’s home. When exemptions eventually wear off (e.g., children or a spouse no longer live in the home), the government collects the cost incurred by Medicaid to enable us, as a country, to provide Medicaid support to other needy individuals. Essentially, Medicaid LTC benefits are a long-term interest-free loan which is forgiven if there is no ability to repay.
The state is reimbursed for LTC services and related prescription drugs and hospital costs. The state may also recover any Medicare cost-sharing and non-LTC Medicaid costs.
Medicaid-planning attorneys help people protect assets for their beneficiaries (children or non-profits). There is an on-going ‘cat and mouse game’ as attorneys find ways to protect assets and legislators and regulators plug what they perceive to be loopholes.
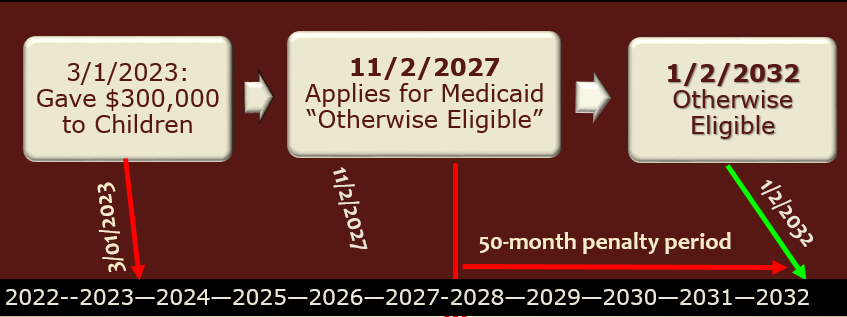
Current law looks back five years (30 months in California, which also restricts estate recovery in several other ways) at any transfers that were made without adequate “consideration”. If such transfers are found, the amount of such transfer is divided by the jurisdiction-specific average daily or monthly cost of care to determine how long the person must wait to qualify for Medicaid service. The following chart show how this works, assuming that the monthly cost of care is $6,000.
How the Partnership Helps
Because you have a LTCi policy, you are unlikely to need Medicaid to pay for your LTC. The government benefits in the ways described at the beginning of this article.
The purchaser of the policy also benefits by not having to qualify for Medicaid. But what if you are very unlucky and use up your LTCi policy and still need LTC? Partnership programs provide an additional back-end protection (additional to Medicaid) under such circumstances.
You can keep $1 of your ‘nest egg’ for every $1 you get from a Partnership-qualified LTCi policy. This concept is called “Asset Disregard” and also “Asset Protection”. Thus, you can qualify for Medicaid without having to spend that money first and that money is also disregarded by the state after you die. This is also described as “Dollar-for-Dollar”. Partnership policies in New York and some Indiana Partnership policies allow all assets to be disregarded (called “Total Asset Disregard”), even beyond the benefits paid by the Partnership LTCi policy.
The Partnership allows a LTCi policy to protect your money twice.
- It pays for your care, saving you money
- It allows you to avoid having to spend that money “down” to qualify for Medicaid.
In the example at the beginning of the article, the insured individual collected $418,836 from the LTCi policy, which then expired. Presuming that the person continues to need care, can they qualify for Medicaid?
If their countable assets are less than or equal to $420,836 and they satisfy above-mentioned qualification requirements, they can qualify for Medicaid immediately. The $420,836 figure reflects their $418,836 expenditure plus the presumed $2,000 jurisdiction-specific exclusion.
With $450,000 of countable assets, you’d have to spend $29,164 of your own money before you might qualify for Medicaid. That wouldn’t take very long.
What if you have $1,300,000 of countable assets? Then, you must spend $879,164 in addition to the $418,836 already spent (plus the amount you spent during the elimination period or because your monthly maximum benefit was insufficient or for non-covered services) before you could qualify for Medicaid.
Spending an additional $879,164 on your care is very unlikely. So, someone with $1,300,000 of countable assets is not likely to qualify for Medicaid. Furthermore, it would take years to spend that additional $879,164. During that period of time, your assets wouldn’t deplete quickly because of your social security, pension, and investment income, RMDs, etc. The $1.3 million in assets is likely to generate $40,000 to $65,000 of income. You’d also have to spend that additional income before you could qualify for Medicaid. That’s a HUGE amount. You’d likely die before spending so much.
This example should make it clear that the Partnership is not a boondoggle for the rich. Some critics think the rich somehow know exactly how much assets they’ll have so they can buy an amount of insurance that will be exactly what they need to allow all their assets to be disregarded. (This would also require that they know when they will need care and how much it will cost.)
Of course, people can’t predict such things accurately so there is an inefficiency in their LTCi planning as they will either buy too little or too much coverage.
More fundamentally, if the rich were so clairvoyant, they would have a huge amount of LTCi that they would be very unlikely to use up. And they’d still have to contribute their income to the cost of their LTC.
Thus, even such clairvoyant people would be unable to game the system meaningfully.
Although this example assumes that the Partnership policy had been totally depleted (expired), in most jurisdictions it is possible to qualify for Medicaid while the Partnership policy is still effective. If past claims create a total Asset Disregard that exceeds countable assets and the policy benefits are insufficient to cover the full cost of care, the policyholder may be eligible for Medicaid help.
In Indiana, Partnership-qualified LTCi policies qualify for a state income tax deduction, but non-Partnership LTCi policies do not qualify for that tax deduction. In other jurisdictions and with the Federal government, tax considerations are the same for Partnership and non-Partnership policies.
Partnership policy qualification requirements
To qualify for Partnership status, the policy must be tax-qualified.
They must also have numerous consumer protections, many of which are required for tax-qualified status and/or for LTCi policies by state regulation.
Legislators have wanted to assure that LTCi coverage stays meaningful as the insured person ages. Compounding the benefit by 5% each year (before claim and while on claim) is expected to do a good job of maintaining purchasing power. Therefore, a level premium 5% compound increase feature is a “safe haven”, guaranteeing that the policy will satisfy the compounding requirement.
Compounding according to a Consumer Price Index qualifies for Partnership except in Kentucky. Level premium 3% compounding qualifies except below age 75 in Idaho.
A provision which applies such compounding to premiums as well as benefits (i.e., is not a level premium approach) qualifies for Partnership status except in KY, PA and SD.
However, future purchase options which charge an attained age price for each slice of additional coverage generally do not qualify for Partnership status.
At least twenty-nine jurisdictions allow level premium 1% compounding to qualify for Partnership status. (AL, AR, AZ, CO, FL, GA, ID, KS, LA, MD, ME, MI, MN, MT, NE, NH, NM, NV, NJ, NC, ND, OK, PA, RI, SD, TN, TX, WV, WY. This can help low-budget buyers qualify for Partnership and also enable employers to pay for a core program so their employees have Partnership-qualified coverage. A higher percentage of policies will qualify for Partnership in the future if insurers and advisors leverage these opportunities. Currently only four insurers offer 1% compounding (CareScout, LifeSecure, Mutual of Omaha and Thrivent).
The original Partnership states (CA, CT, IN, NY) and South Dakota ($100/day) have minimum size requirements for Partnership policies. The original states’ size requirements increase, typically annually. Indiana’s 2025 requirement is low ($115/day) and if the coverage pool is at least $522,686 at issue, total asset disregard applies. The higher minimum size requirements in CA, CT and NY contribute to the lack of Partnership sales in those jurisdictions.
Advisor LTCi Certification
The DRA also established a requirement that agents selling Partnership policies have suitable training. The NAIC, in drafting a model Partnership regulation, required such training to sell all LTCi policies. It wanted to encourage all LTCi salespeople to have training.
Some states adopted the DRA wording while others adopted the NAIC wording, one way in which standards vary by jurisdiction. In states with the NAIC wording, certification is also required to sell linked-benefit policies with §7702B wording. Policies with chronic illness (§101g) wording, rather than §7702B “LTCi” wording, can be sold by agents who are not certified.
Most states require 8-hour training up-front and 4-hour renewals every 2 years. Doing such training in one state is sufficient to qualify in all such states. However, some states have unique training requirements. The original 4 Partn ership states (CA, CT, IN and NY) have their own training requirements. CO requires 16-hour training up-front and 5-hour renewals for domestic agents. Several states (such as GA, MA, MN, SD, VA, VT, WI) require a one- or two-hour supplement that addresses state-specific Partnership and/or Medicaid rules. (In these states, the basic training is accepted, but the supplement is required.)
Although certification renewal every two years is standard, the measurement of the two-year period varies by jurisdiction. Many jurisdictions require that the training be done once in every renewal licensing cycle. In such states, an agent might remain qualified to sell LTCi even if they have gone nearly four years without re-certifying. (They could have taken the certification class early in one cycle, then late in the next.) However, some insurers balk at accepting applications if the agent has not taken the certification class in the two-year period prior to the date the application is signed.
Twenty-one states require that re-certification occur within two years of the previous certification. In these jurisdictions, if an agent takes the certification class earlier than necessary, they have to take every future re-certification class earlier.
An agent’s failure to maintain certification can be damaging to the agent’s clients. Insurers fear being fined if they accept an application from an agent whose certification is out-of-date. Thus, they require the agent to get certified, then take a new application. The following problems can occur:
- A health change may can the applicant to no longer be insurable or to be placed in a less favorable class.
- The client may have had a birthday that causes them to be too old to qualify for coverage.
- An age change can cause the applicant to have a higher premium forever into the future.
- A product may no longer be available or may have become less attractive.
- The applicant may no longer be married or may get fewer years of tax break.
- The applicant will have lower benefits at claim time because compounding will be delayed and perhaps one less future purchase option may be offered prior to claim.
- Some benefits, like survivorship and sometimes return of premium on death, require that the policy have been in force for 10 years. An applicant may end up not qualifying for such a benefit because of the later date of the second app.
- The client also has the nuisance of a new app.
In addition to the client problems and potential liability, delay can also be a nuisance for the broker because it can require taking the 8-hour class again (Illinois requires a new 8-hour exam if renewal occurs 12 or more months too late and Virginia requires a new 8-hour exam if renewal is just one day late.
Advisors can ask the state to put in writing that, to avoid consumer disadvantage, it is OK for the insurer to accept the application despite certification having been completed after the date of the application. With such assurance, insurers will sometimes accommodate the applicant.
Partnership Success
Prior to the Deficit Reduction Act, Partnerships for long-term care insurance were available only in CA, CT, IN, and NY. Their success seems clear because 13.2% of the individual LTCi policies in the USA were sold in those 4 Partnership states in 1993, before the Partnerships were effective, but 19.4% of the policies in 2007 (and 24.1% of the premium) were sold in those states. What would have caused that increased market share other than the Partnerships?
However, since then, LTCi has become much more expensive. The Partnership target market has a much tougher time trying to afford coverage.
The table below shows, for each jurisdiction, the percentage of 2024 sales that qualified for the Partnership and the average premium per insured (for all policies and just for Partnership policies; these average premiums are distorted by including FPOs and 100% of single premiums).
Traditionally, north central states such as Minnesota, North Dakota, and Wisconsin have had a high percentage of policies qualify for Partnership. The restrictive requirements of the four original Partnership states has resulted in no Partnership sales being reported in 2024 in California, Connecti
| Jurisdiction | % qualified | Average Premium including FPOs and full Single Premium | |
| For Partnership | Total | Partnership | |
| Alabama | 20.1% | $5,139.29 | $3,829.03 |
| Alaska | 0.0% | $5,008.13 | |
| Arizona | 39.1% | $4,916.26 | $6,288.26 |
| Arkansas | 19.5% | $4,514.11 | $5,707.61 |
| California | 0.0% | $5,085.68 | |
| Colorado | 32.7% | $5,192.62 | $5,110.70 |
| Connecticut | 0.0% | $4,942.90 | |
| District of Columbia | 0.0% | $4,826.74 | |
| Delaware | 17.2% | $4,254.30 | $4,464.19 |
| Florida | 20.0% | $3,800.33 | $3,969.00 |
| Georgia | 43.5% | $5,010.28 | $5,896.17 |
| Hawaii | 0.0% | $3,542.03 | |
| Idaho | 27.3% | $5,177.34 | $5,543.61 |
| Illinois | 25.7% | $6,026.78 | $5,402.07 |
| Indiana | 2.2% | $4,361.52 | $4,345.00 |
| Iowa | 48.7% | $4,619.13 | $5,781.95 |
| Kansas | 35.3% | $3,677.07 | $4,739.14 |
| Kentucky | 20.2% | $3,668.27 | $6,870.04 |
| Louisiana | 31.3% | $4,581.23 | $6,733.14 |
| Maine | 13.2% | $4,140.79 | $4,881.78 |
| Maryland | 29.5% | $5,079.68 | $4,002.57 |
| Massachusetts | 0.0% | $6,509.52 | |
| Michigan | 23.5% | $3,615.51 | $3,716.26 |
| Minnesota | 62.2% | $4,453.43 | $5,257.07 |
| Mississippi | 0.0% | $5,973.75 | |
| Missouri | 19.6% | $4,135.87 | $5,537.02 |
| Montana | 31.5% | $3,763.96 | $4,294.08 |
| Nebraska | 47.9% | $4,596.42 | $6,018.41 |
| Nevada | 44.7% | $3,873.18 | $4,236.62 |
| New Hampshire | 24.4% | $4,479.23 | $3,690.45 |
| New Jersey | 15.4% | $3,958.01 | $5,343.11 |
| New Mexico | 12.8% | $6,205.18 | $4,358.84 |
| New York | 0.0% | $6,025.40 | |
| North Carolina | 37.6% | $4,326.59 | $6,417.17 |
| North Dakota | 62.0% | $4,296.13 | $4,653.20 |
| Ohio | 55.1% | $4,949.35 | $6,113.57 |
| Oklahoma | 35.3% | $4,638.05 | $6,987.64 |
| Oregon | 51.8% | $6,650.21 | $8,533.18 |
| Pennsylvania | 19.6% | $4,802.45 | $4,534.44 |
| Puerto Rico | 0.0% | $874.83 | |
| Rhode Island | 28.2% | $4,361.46 | $6,855.65 |
| South Carolina | 35.3% | $4,141.82 | $5,935.71 |
| South Dakota | 51.1% | $6,506.58 | $7,089.57 |
| Tennessee | 38.6% | $4,700.81 | $6,851.20 |
| Texas | 19.7% | $3,888.70 | $3,912.12 |
| Utah | 0.0% | $5,462.42 | |
| Vermont | 0.0% | $5,381.62 | |
| Virginia | 30.6% | $4,568.10 | $6,437.06 |
| Washington | 27.2% | $4,134.90 | $4,578.07 |
| West Virginia | 8.8% | $2,853.16 | $3,063.89 |
| Wisconsin | 62.8% | $5,023.45 | $5,697.89 |
| Wyoming | 30.8% | $5,350.37 | $10,871.57 |
| Total | 26.9% | $4,654.18 | $5,499.52 |
Participants reported Partnership sales in 41 states, all Partnership-authorized states except CA, CT and NY. Only one insurer sells Partnership in IN; that insurer issued Partnership policies in 41 states. One insurer issues no Partnership policies.
Overall, 26.9% of policies qualified for Partnership, but 33.5% of policies qualified for Partnership in the DRA states (38.9% excluding Bankers’ Fundamental Plus product). Excluding Bankers’ Fundamental Plus product, 80% of Minnesota’s policies and 74% of Wisconsin’s policies qualified for Partnership, but 5 DRA states had less than 20% qualify.
Partnership programs could be more effective if:
- Advisors offer small maximum monthly benefits more frequently to middle-income individuals and stress the importance of benefit increases to maintain LTCI purchasing power and qualify for Partnership asset disregard. For example, a $1,500 initial maximum monthly benefit covers about 1.5 hours of home care per day and, with compound benefit increases, may maintain buying power. Many middle-income individuals would like LTCI to help them stay at home while not “burning out” family caregivers and could be motivated further by Partnership asset disregard. (This approach does not work in CA, CT, IN and NY because of their high Partnership minimum daily benefit requirements.)
- The four original Partnership states migrate to DRA rules. That would make it easier for policies to qualify for the Partnership in those four states and would create more uniformity. Uniformity would simplify the process for agents and general agents and encourage Partnership sales in multi-jurisdiction employer sales.
- AK, HI, MA, MS, VT, and DC adopt Partnership programs.
- Programs that privately finance direct mail educational LTCI content from public agencies were adopted more broadly.
- Financial advisors press reluctant insurers to certify their products and offer 1% compounding.
- More financial advisors were LTCI-certified. Some people argue that certification requirements should be loosened. Certainly re-certification rules could be improved in some jurisdictions.
- Linked-benefit products became Partnership-qualified.
- All Partnership jurisdictions honored asset disregard accumulated in other jurisdictions. The DRA established reciprocity unless a state opted out and permits states to opt out in the future even if they recognize reciprocity today. Except for California and for New York relative to policies not approved in NY, states with Partnership programs currently grant reciprocity to asset disregard from policies issued in other jurisdictions.
- Reciprocity in agent certification was more common. California does not recognize out-of-state certification.
- All states guaranteed asset disregard. Some states retain the right to deny asset disregard at any time in the future, including disavowing past asset disregard accumulations. I am not aware that such uncertainty has harmed the market, but ‘bait and switch’ practices are unbecoming. Ironically, a state which guarantees asset disregard requires that applicants be notified that asset disregard is not guaranteed. (This happened because they copied the disclosure requirement of a state that does not guarantee asset disregard.)


