Claude Thau is president of Thau Inc., and works to help build a sound long term care insurance industry. Thau wholesales long term care-related products for brokers nationwide as Marketing Manager at BackNine Insurance. In addition to his duties at BackNine, Thau consults for insurers, consulting firms, regulators, etc., creates unique software to help advisors educate clients, and does LTCI and long term care pro bono work, as LTCI’s value relies on quality long term care being available.
He also sells a little LTCI himself, as current sales experience is important to be a good wholesaler and consultant.
Thau’s LTCI experience is unusually broad and deep. After a career as an actuary, he led a major insurer’s LTCI division, which then grew five times as fast as the rest of the LTCI industry for each of three consecutive years. Since setting up Thau, Inc. in 2000, he has consulted for the Federal government’s LTCI program, chaired the Center for Long-Term Care Financing, and, since 2005, led the Milliman LTCI Survey, published annually in the July and August issues of Broker World.
A former inner-city public school teacher, Thau enjoys mentoring brokers individually to help them grow their business.
Thau can be reached by telephone at 913-707-8863. Email: claude.thau@gmail.com.
The 2025 Milliman Long Term Care Insurance Survey is the 27th consecutive annual review of stand-alone and combination long-term care insurance (LTCI) published by Broker World magazine. This comprehensive report, authored by Claude Thau, Nicole Gaspar, Chris Giese, and Matthew Epps, provides a detailed review of the individual and worksite stand-alone LTCI marketplace, sales distributions, claims, underwriting trends and available products as well as sales and commentary relative to combination LTCi. We thank insurance company staff for submitting the data and responding to questions promptly.
The report includes the following sections and exhibits:
Section IV: Claims Data Analysis – Stand-alone LTCI
Section V: Statistical Analysis of Stand-alone LTCI Sales
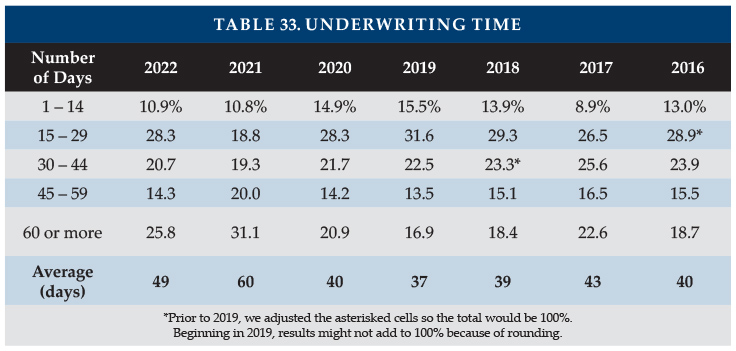
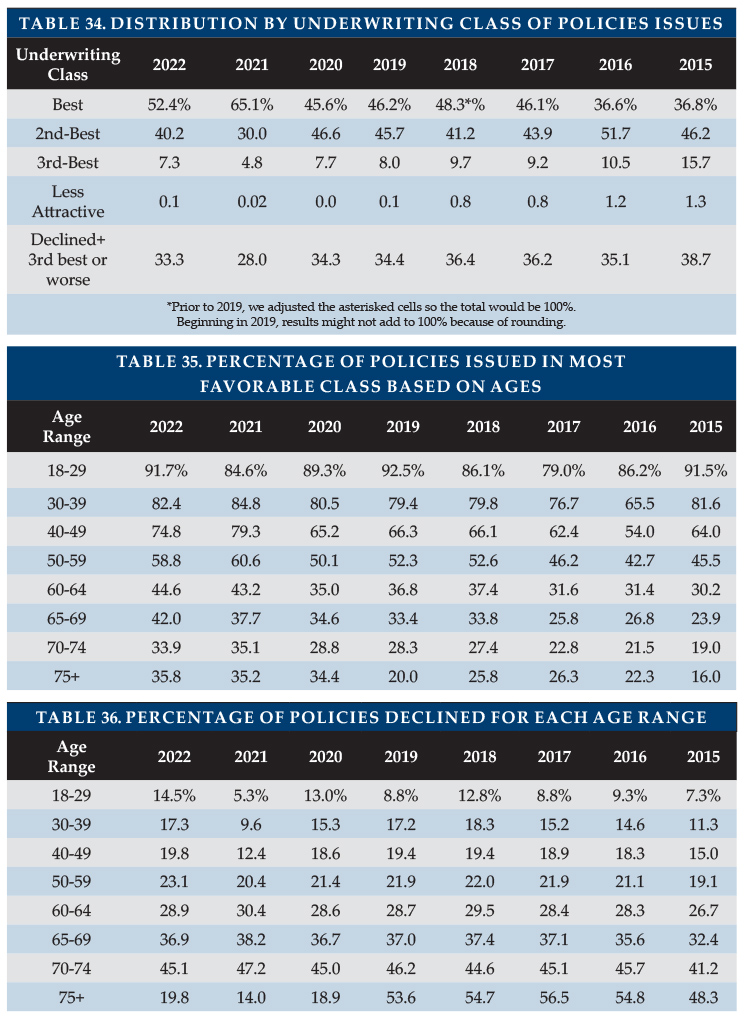
Section VI: Underwriting Data Analysis – Stand-alone LTCI
Stand-Alone LTCi Product Display shows financial ratings, LTCI sales and inforce policies, and generic product details
Stand-Alone LTCi Premium Display includes lifetime annual premiums by insurer for various benefit options
Stand-Alone Underwriting Class Display shows the premium adjustment (from the Premium Display) for each underwriting class and also shows the distribution of issued policies by underwriting class
Dive into the complete 2025 Milliman Long-Term Care Insurance Survey for all the data, analysis, and expert commentary. Read the Full Report
Funding long-term care (LTC) has been recognized as a huge issue for our country for a long time. Insurers, regulators, politicians, providers, educators and policy wonks continue to seek solutions.
For the purposes of this article, let’s assume that a client age 55 buys a Partnership-qualified policy with an initial monthly maximum of $4500, 3% compounding and a 3-year benefit period after a 90-service-day elimination period. Let’s assume the client begins to need qualifying care at age 85½, at which time her maximum monthly benefit would have risen to $11,044. For convenience, I’ll assume the insured/claimant is female and her life partner (if any) is male. If she uses the full amount each month, her LTCi benefits would be as follows:
Insurance Age at the Beginning of the Claim Year
Maximum Monthly Benefit
Number of Months of Benefits Paid
Reimbursement of that Year’s Expenses
Comment
85
$11,044
3
$33,132
Claim started at mid-year; 90-day EP; so only 3 months paid
86
$11,375
12
$136,500
87
$11,717
12
$140,592
88
$12,068
9
$108,612
Total
$418,836
The government benefits from that purchase of private LTCi in the following ways:
The private insurance LTCi benefit of $418,836 likely kept the client off Medicaid or contributed to the cost of Medicaid care, saving money for both the Federal government and state government.
For those kept off Medicaid, the state avoids the administrative cost of determining whether the insured is eligible for Medicaid, setting up records, and making payments.
The state and Federal governments benefit because LTC providers get the full private pay rate rather than the reduced Medicaid rate. Providers are therefore better able to provide outstanding service. The more LTCi there is, the more likely it is that innovators will want to be in the LTC industry, providing new and better services.
The additional revenue enables the provider to earn more profit and/or pay higher salaries. Thus, the provider and/or its employees pay higher income taxes to the state and Federal governments.
With LTCi, the client is likely to be less dependent on family care. Thus, family members are likely to be more productive for society and to generate more income, which results in more income taxes for state and Federal governments.
The insurance agent who sold LTCi will pay income taxes on his/her commissions to the state and Federal governments.
The insurance company will pay premium tax to the state and income tax to the Federal government.
As noted in the above bullets, the insured person benefits, the insured’s family benefits, the providers and their employees benefit, insurance brokers and their families benefit, and insurers (and their employees and shareholders) benefit, as well as the state and Federal government.
The Robert Woods Johnson Foundation (Mark Meiners, in particular) brainstormed to find a way to protect the government from the LTC costs of an aging population. What could the government do to encourage the middle class to buy more LTCi? They developed a win-win-win-win-win-win concept to make private long-term care insurance (LTCi) more affordable for the middle class: State/Carriers Public Partnerships. In a nutshell, State Partnerships are an additional back-end safety net to reward middle-class people for buying LTCi.
Four states (CA, CT, IN and NY) blazed the trail for Partnership programs in the early 1990s. However, an aide to Congressman Henry Waxman incorrectly concluded that the Partnership was a boondoggle for the rich. So, Waxman inserted into Federal legislation (OBRA, 1993) a provision prohibiting other states from developing future Partnerships. The four existing programs (including his state, CA) were grandfathered.
Twelve years later, the Deficit Reduction Act of 2005 (DRA) removed the restriction, allowing more jurisdictions to create Partnership programs. Now, 45 states have Partnership programs. (Partnership policies are not available in AK, HI, MA, MS, or VT, nor in DC, Puerto Rico or Guam. However, MA has a similar program called MassHealth Exemption.) The original, grandfathered states’ provisions differ among themselves and also differ from the provisions of the other 41 “DRA” states. There are also slight differences among the DRA states, most particularly relative to what types of compound benefit provisions can qualify for Partnership status.
Medicaid Eligibility in General
When our claimant applies to Medicaid for long-term care services, state reviewers determine whether she is eligible for Medicaid (“Medi-Cal” in California) LTC benefits. The numbers in this section of the article apply in 2025, unless otherwise indicated.
Any of her income in excess of $50/month (varies by state and may differ for home care) must be applied to the cost of care. If that income is sufficient to cover her entire cost of care, she is not eligible for Medicaid. Notes:
Her spouse is entitled to his independent income (however, if he owns an annuity in payout mode that has a certain period or death benefit, the state must be identified as a secondary beneficiary.
If her spouse is impoverished, she can transfer income to him to bring his income up to $2,555/month. He can appeal to get as much as $3,948/month, so some jurisdictions (AK, CA, DC, GA, IL, IA, LA, MS, NV, NY, OK, SC, TX, WY) automatically permit up to $3,948 instead of $2,555.
Some states have an “income cap” ($2,901/month) rather than determining whether the income is sufficient to cover the cost of care. That is, if your income exceeds $2,901/month, you are ineligible for Medicaid LTC support. People who can’t afford their LTC but who earn too much income can put excess income into a Miller Trust which pays their provider. That brings their income within limits, qualifying them for Medicaid if they and their trust were unable to pay the full cost..
In jurisdictions other than California, the care-needy individual must also apply “countable assets” in excess of $2,000 (in most states) toward the cost of care.
Non-countable assets include:
The person’s home (unless equity exceeds the amount shown below) if any of the following circumstances apply
The person may return to the home
The person’s spouse is living in the home
The person’s child under age 21 or blind or permanently & totally disabled is living in the home
A sibling is living in the home and resided in it for at least one year (while having an ownership interest) immediately before the person was admitted to the facility.
A child is living in the home and resided in home for at least two years immediately before the person’s admission and provided care which permitted the person to stay home rather than be in an institution.
The person is ineligible for Medicaid if home equity exceeds $730,000, except that the cap is $1,097,000 in CO, CT, DC, HI, MA, NJ, NY, and WA. (CA does not impose this limitation.) These limits are indexed each year.
One automobile
Household and personal belongings
Wedding and engagement rings
Income-generating property (because the income must be used to pay for care)
Burial plot and prepaid burial plans
Cash value of life insurance if, and only if, the combined death benefit under such policies is less than 1500.
Term insurance
To be clear “countable assets” include:
Cash above the limit ($2000 or so for single people; $3000 or so for a couple who both need care)
Other liquid assets: CDs, T-bills, stocks, bonds, retirement accounts (Keough*, 4.01k*, IRA*, 4.03b, etc.). Kansas is an exception in that the spouse’s §4.03B funds are exempt.
Cash Value of life insurance if the combined death benefits exceeds $1500
Vacation home
Second vehicles
Medicaid Repayment
Federal legislation (Public Law 104-191) requires that Medicaid costs be reimbursed by the recipient’s estate (“estate recovery”). When someone begins to need Medicaid support for LTC, the state may place a lien on that person’s home. When exemptions eventually wear off (e.g., children or a spouse no longer live in the home), the government collects the cost incurred by Medicaid to enable us, as a country, to provide Medicaid support to other needy individuals. Essentially, Medicaid LTC benefits are a long-term interest-free loan which is forgiven if there is no ability to repay.
The state is reimbursed for LTC services and related prescription drugs and hospital costs. The state may also recover any Medicare cost-sharing and non-LTC Medicaid costs.
Medicaid-planning attorneys help people protect assets for their beneficiaries (children or non-profits). There is an on-going ‘cat and mouse game’ as attorneys find ways to protect assets and legislators and regulators plug what they perceive to be loopholes.
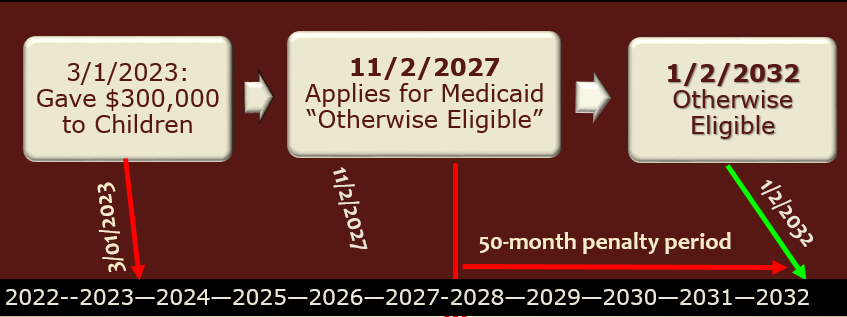
Current law looks back five years (30 months in California, which also restricts estate recovery in several other ways) at any transfers that were made without adequate “consideration”. If such transfers are found, the amount of such transfer is divided by the jurisdiction-specific average daily or monthly cost of care to determine how long the person must wait to qualify for Medicaid service. The following chart show how this works, assuming that the monthly cost of care is $6,000.
How the Partnership Helps
Because you have a LTCi policy, you are unlikely to need Medicaid to pay for your LTC. The government benefits in the ways described at the beginning of this article.
The purchaser of the policy also benefits by not having to qualify for Medicaid. But what if you are very unlucky and use up your LTCi policy and still need LTC? Partnership programs provide an additional back-end protection (additional to Medicaid) under such circumstances.
You can keep $1 of your ‘nest egg’ for every $1 you get from a Partnership-qualified LTCi policy. This concept is called “Asset Disregard” and also “Asset Protection”. Thus, you can qualify for Medicaid without having to spend that money first and that money is also disregarded by the state after you die. This is also described as “Dollar-for-Dollar”. Partnership policies in New York and some Indiana Partnership policies allow all assets to be disregarded (called “Total Asset Disregard”), even beyond the benefits paid by the Partnership LTCi policy.
The Partnership allows a LTCi policy to protect your money twice.
It pays for your care, saving you money
It allows you to avoid having to spend that money “down” to qualify for Medicaid.
In the example at the beginning of the article, the insured individual collected $418,836 from the LTCi policy, which then expired. Presuming that the person continues to need care, can they qualify for Medicaid?
If their countable assets are less than or equal to $420,836 and they satisfy above-mentioned qualification requirements, they can qualify for Medicaid immediately. The $420,836 figure reflects their $418,836 expenditure plus the presumed $2,000 jurisdiction-specific exclusion.
With $450,000 of countable assets, you’d have to spend $29,164 of your own money before you might qualify for Medicaid. That wouldn’t take very long.
What if you have $1,300,000 of countable assets? Then, you must spend $879,164 in addition to the $418,836 already spent (plus the amount you spent during the elimination period or because your monthly maximum benefit was insufficient or for non-covered services) before you could qualify for Medicaid.
Spending an additional $879,164 on your care is very unlikely. So, someone with $1,300,000 of countable assets is not likely to qualify for Medicaid. Furthermore, it would take years to spend that additional $879,164. During that period of time, your assets wouldn’t deplete quickly because of your social security, pension, and investment income, RMDs, etc. The $1.3 million in assets is likely to generate $40,000 to $65,000 of income. You’d also have to spend that additional income before you could qualify for Medicaid. That’s a HUGE amount. You’d likely die before spending so much.
This example should make it clear that the Partnership is not a boondoggle for the rich. Some critics think the rich somehow know exactly how much assets they’ll have so they can buy an amount of insurance that will be exactly what they need to allow all their assets to be disregarded. (This would also require that they know when they will need care and how much it will cost.)
Of course, people can’t predict such things accurately so there is an inefficiency in their LTCi planning as they will either buy too little or too much coverage.
More fundamentally, if the rich were so clairvoyant, they would have a huge amount of LTCi that they would be very unlikely to use up. And they’d still have to contribute their income to the cost of their LTC.
Thus, even such clairvoyant people would be unable to game the system meaningfully.
Although this example assumes that the Partnership policy had been totally depleted (expired), in most jurisdictions it is possible to qualify for Medicaid while the Partnership policy is still effective. If past claims create a total Asset Disregard that exceeds countable assets and the policy benefits are insufficient to cover the full cost of care, the policyholder may be eligible for Medicaid help.
In Indiana, Partnership-qualified LTCi policies qualify for a state income tax deduction, but non-Partnership LTCi policies do not qualify for that tax deduction. In other jurisdictions and with the Federal government, tax considerations are the same for Partnership and non-Partnership policies.
Partnership policy qualification requirements
To qualify for Partnership status, the policy must be tax-qualified.
They must also have numerous consumer protections, many of which are required for tax-qualified status and/or for LTCi policies by state regulation.
Legislators have wanted to assure that LTCi coverage stays meaningful as the insured person ages. Compounding the benefit by 5% each year (before claim and while on claim) is expected to do a good job of maintaining purchasing power. Therefore, a level premium 5% compound increase feature is a “safe haven”, guaranteeing that the policy will satisfy the compounding requirement.
Compounding according to a Consumer Price Index qualifies for Partnership except in Kentucky. Level premium 3% compounding qualifies except below age 75 in Idaho.
A provision which applies such compounding to premiums as well as benefits (i.e., is not a level premium approach) qualifies for Partnership status except in KY, PA and SD.
However, future purchase options which charge an attained age price for each slice of additional coverage generally do not qualify for Partnership status.
At least twenty-nine jurisdictions allow level premium 1% compounding to qualify for Partnership status. (AL, AR, AZ, CO, FL, GA, ID, KS, LA, MD, ME, MI, MN, MT, NE, NH, NM, NV, NJ, NC, ND, OK, PA, RI, SD, TN, TX, WV, WY. This can help low-budget buyers qualify for Partnership and also enable employers to pay for a core program so their employees have Partnership-qualified coverage. A higher percentage of policies will qualify for Partnership in the future if insurers and advisors leverage these opportunities. Currently only four insurers offer 1% compounding (CareScout, LifeSecure, Mutual of Omaha and Thrivent).
The original Partnership states (CA, CT, IN, NY) and South Dakota ($100/day) have minimum size requirements for Partnership policies. The original states’ size requirements increase, typically annually. Indiana’s 2025 requirement is low ($115/day) and if the coverage pool is at least $522,686 at issue, total asset disregard applies. The higher minimum size requirements in CA, CT and NY contribute to the lack of Partnership sales in those jurisdictions.
Advisor LTCi Certification
The DRA also established a requirement that agents selling Partnership policies have suitable training. The NAIC, in drafting a model Partnership regulation, required such training to sell all LTCi policies. It wanted to encourage all LTCi salespeople to have training.
Some states adopted the DRA wording while others adopted the NAIC wording, one way in which standards vary by jurisdiction. In states with the NAIC wording, certification is also required to sell linked-benefit policies with §7702B wording. Policies with chronic illness (§101g) wording, rather than §7702B “LTCi” wording, can be sold by agents who are not certified.
Most states require 8-hour training up-front and 4-hour renewals every 2 years. Doing such training in one state is sufficient to qualify in all such states. However, some states have unique training requirements. The original 4 Partn ership states (CA, CT, IN and NY) have their own training requirements. CO requires 16-hour training up-front and 5-hour renewals for domestic agents. Several states (such as GA,MA, MN, SD, VA, VT, WI) require a one- or two-hour supplement that addresses state-specific Partnership and/or Medicaid rules. (In these states, the basic training is accepted, but the supplement is required.)
Although certification renewal every two years is standard, the measurement of the two-year period varies by jurisdiction. Many jurisdictions require that the training be done once in every renewal licensing cycle. In such states, an agent might remain qualified to sell LTCi even if they have gone nearly four years without re-certifying. (They could have taken the certification class early in one cycle, then late in the next.) However, some insurers balk at accepting applications if the agent has not taken the certification class in the two-year period prior to the date the application is signed.
Twenty-one states require that re-certification occur within two years of the previous certification. In these jurisdictions, if an agent takes the certification class earlier than necessary, they have to take every future re-certification class earlier.
An agent’s failure to maintain certification can be damaging to the agent’s clients. Insurers fear being fined if they accept an application from an agent whose certification is out-of-date. Thus, they require the agent to get certified, then take a new application. The following problems can occur:
A health change may can the applicant to no longer be insurable or to be placed in a less favorable class.
The client may have had a birthday that causes them to be too old to qualify for coverage.
An age change can cause the applicant to have a higher premium forever into the future.
A product may no longer be available or may have become less attractive.
The applicant may no longer be married or may get fewer years of tax break.
The applicant will have lower benefits at claim time because compounding will be delayed and perhaps one less future purchase option may be offered prior to claim.
Some benefits, like survivorship and sometimes return of premium on death, require that the policy have been in force for 10 years. An applicant may end up not qualifying for such a benefit because of the later date of the second app.
The client also has the nuisance of a new app.
In addition to the client problems and potential liability, delay can also be a nuisance for the broker because it can require taking the 8-hour class again (Illinois requires a new 8-hour exam if renewal occurs 12 or more months too late and Virginia requires a new 8-hour exam if renewal is just one day late.
Advisors can ask the state to put in writing that, to avoid consumer disadvantage, it is OK for the insurer to accept the application despite certification having been completed after the date of the application. With such assurance, insurers will sometimes accommodate the applicant.
Partnership Success
Prior to the Deficit Reduction Act, Partnerships for long-term care insurance were available only in CA, CT, IN, and NY. Their success seems clear because 13.2% of the individual LTCi policies in the USA were sold in those 4 Partnership states in 1993, before the Partnerships were effective, but 19.4% of the policies in 2007 (and 24.1% of the premium) were sold in those states. What would have caused that increased market share other than the Partnerships?
However, since then, LTCi has become much more expensive. The Partnership target market has a much tougher time trying to afford coverage.
The table below shows, for each jurisdiction, the percentage of 2024 sales that qualified for the Partnership and the average premium per insured (for all policies and just for Partnership policies; these average premiums are distorted by including FPOs and 100% of single premiums).
Traditionally, north central states such as Minnesota, North Dakota, and Wisconsin have had a high percentage of policies qualify for Partnership. The restrictive requirements of the four original Partnership states has resulted in no Partnership sales being reported in 2024 in California, Connecti
Jurisdiction
% qualified
Average Premium including FPOs and full Single Premium
For Partnership
Total
Partnership
Alabama
20.1%
$5,139.29
$3,829.03
Alaska
0.0%
$5,008.13
Arizona
39.1%
$4,916.26
$6,288.26
Arkansas
19.5%
$4,514.11
$5,707.61
California
0.0%
$5,085.68
Colorado
32.7%
$5,192.62
$5,110.70
Connecticut
0.0%
$4,942.90
District of Columbia
0.0%
$4,826.74
Delaware
17.2%
$4,254.30
$4,464.19
Florida
20.0%
$3,800.33
$3,969.00
Georgia
43.5%
$5,010.28
$5,896.17
Hawaii
0.0%
$3,542.03
Idaho
27.3%
$5,177.34
$5,543.61
Illinois
25.7%
$6,026.78
$5,402.07
Indiana
2.2%
$4,361.52
$4,345.00
Iowa
48.7%
$4,619.13
$5,781.95
Kansas
35.3%
$3,677.07
$4,739.14
Kentucky
20.2%
$3,668.27
$6,870.04
Louisiana
31.3%
$4,581.23
$6,733.14
Maine
13.2%
$4,140.79
$4,881.78
Maryland
29.5%
$5,079.68
$4,002.57
Massachusetts
0.0%
$6,509.52
Michigan
23.5%
$3,615.51
$3,716.26
Minnesota
62.2%
$4,453.43
$5,257.07
Mississippi
0.0%
$5,973.75
Missouri
19.6%
$4,135.87
$5,537.02
Montana
31.5%
$3,763.96
$4,294.08
Nebraska
47.9%
$4,596.42
$6,018.41
Nevada
44.7%
$3,873.18
$4,236.62
New Hampshire
24.4%
$4,479.23
$3,690.45
New Jersey
15.4%
$3,958.01
$5,343.11
New Mexico
12.8%
$6,205.18
$4,358.84
New York
0.0%
$6,025.40
North Carolina
37.6%
$4,326.59
$6,417.17
North Dakota
62.0%
$4,296.13
$4,653.20
Ohio
55.1%
$4,949.35
$6,113.57
Oklahoma
35.3%
$4,638.05
$6,987.64
Oregon
51.8%
$6,650.21
$8,533.18
Pennsylvania
19.6%
$4,802.45
$4,534.44
Puerto Rico
0.0%
$874.83
Rhode Island
28.2%
$4,361.46
$6,855.65
South Carolina
35.3%
$4,141.82
$5,935.71
South Dakota
51.1%
$6,506.58
$7,089.57
Tennessee
38.6%
$4,700.81
$6,851.20
Texas
19.7%
$3,888.70
$3,912.12
Utah
0.0%
$5,462.42
Vermont
0.0%
$5,381.62
Virginia
30.6%
$4,568.10
$6,437.06
Washington
27.2%
$4,134.90
$4,578.07
West Virginia
8.8%
$2,853.16
$3,063.89
Wisconsin
62.8%
$5,023.45
$5,697.89
Wyoming
30.8%
$5,350.37
$10,871.57
Total
26.9%
$4,654.18
$5,499.52
Participants reported Partnership sales in 41 states, all Partnership-authorized states except CA, CT and NY. Only one insurer sells Partnership in IN; that insurer issued Partnership policies in 41 states. One insurer issues no Partnership policies.
Overall, 26.9% of policies qualified for Partnership, but 33.5% of policies qualified for Partnership in the DRA states (38.9% excluding Bankers’ Fundamental Plus product). Excluding Bankers’ Fundamental Plus product, 80% of Minnesota’s policies and 74% of Wisconsin’s policies qualified for Partnership, but 5 DRA states had less than 20% qualify.
Partnership programs could be more effective if:
Advisors offer small maximum monthly benefits more frequently to middle-income individuals and stress the importance of benefit increases to maintain LTCI purchasing power and qualify for Partnership asset disregard. For example, a $1,500 initial maximum monthly benefit covers about 1.5 hours of home care per day and, with compound benefit increases, may maintain buying power. Many middle-income individuals would like LTCI to help them stay at home while not “burning out” family caregivers and could be motivated further by Partnership asset disregard. (This approach does not work in CA, CT, IN and NY because of their high Partnership minimum daily benefit requirements.)
The four original Partnership states migrate to DRA rules. That would make it easier for policies to qualify for the Partnership in those four states and would create more uniformity. Uniformity would simplify the process for agents and general agents and encourage Partnership sales in multi-jurisdiction employer sales.
AK, HI, MA, MS, VT, and DC adopt Partnership programs.
Programs that privately finance direct mail educational LTCI content from public agencies were adopted more broadly.
Financial advisors press reluctant insurers to certify their products and offer 1% compounding.
More financial advisors were LTCI-certified. Some people argue that certification requirements should be loosened. Certainly re-certification rules could be improved in some jurisdictions.
Linked-benefit products became Partnership-qualified.
All Partnership jurisdictions honored asset disregard accumulated in other jurisdictions. The DRA established reciprocity unless a state opted out and permits states to opt out in the future even if they recognize reciprocity today. Except for California and for New York relative to policies not approved in NY, states with Partnership programs currently grant reciprocity to asset disregard from policies issued in other jurisdictions.
Reciprocity in agent certification was more common. California does not recognize out-of-state certification.
All states guaranteed asset disregard. Some states retain the right to deny asset disregard at any time in the future, including disavowing past asset disregard accumulations. I am not aware that such uncertainty has harmed the market, but ‘bait and switch’ practices are unbecoming. Ironically, a state which guarantees asset disregard requires that applicants be notified that asset disregard is not guaranteed. (This happened because they copied the disclosure requirement of a state that does not guarantee asset disregard.)
They are your clients, and they will have questions. Naturally, your inclination is to help—even if they didn’t purchase the long-term care policy from you. Instead, first stop. Stop, to avoid overcommitting. To be clear, the point of stopping is not for clients to delay submitting their claim. The point is to be thoughtful and prudent before acting. Has your client even reviewed the policy before calling in the claim? Will you be assisting them? The goal is to produce a good experience for them and to avoid the hassle and stress associated with a delayed or denied claim.
If the insured or family member reaches out telling you they think it’s time to go on claim, listen. Listen and empathize as they describe their challenges and the strain on their family. Then, take a moment to praise the decision to purchase the policy to begin with. They already have a great head start compared to most Americans. Even so, it’s important to convey the process they are about to embark on.
Understanding Eligibility A long-term care insurance (LTCi) policy is catastrophic coverage, comparable to homeowner’s insurance. The homeowner’s policy kicks in when the house is destroyed by a fire or tornado. But it won’t pay for home maintenance and repairs.
Similarly, LTCi is not designed to help with all the afflictions of growing old. Generally, insureds need support before they can satisfy the criteria to receive LTCi benefits from their policy. They will likely need help with Instrumental Activities of Daily Living (IADLs) like food preparation, grocery shopping, housekeeping, managing medications, managing finances, paying bills, yard work, or transportation.
When they think they are eligible to be on claim, a licensed health care practitioner (doctor, nurse, social worker) will assess whether they satisfy the eligibility criteria (i.e. triggers). Generally, this is (1) having a severe cognitive impairment or (2) needing help, from another person, with at least 2 out of 6 activities of daily living (ADLs) like bathing, dressing, toileting, transferring (in and out of bed or chair), eating, and continence. Once the criteria have been met, the LTCi policy can cover IADLs as well.
Note: Most policies consider ADLs to include standby assistance as well as hands-on assistance. Also, older LTCi policies issued before 1993, may have language requiring hospitalization or nursing home stay before benefit eligibility.
Common Reasons for LTC Claims Denials:
Insufficient evidence or documentation to satisfy eligibility
Insufficient documentation for the Plan of Care
Unapproved or unlicensed care provider
Services not covered
Elimination period not met
Policy lapsed
Conflicting medical opinions
Excluded conditions (like substance abuse or self-inflicted injuries)
Manage Expectations–The Process Claims can take eight-plus weeks to get approved when assisted by third parties like: Amada Senior Care, Jahnke Consulting, or Thalheimer Insurance. For unassisted claims it could be eight to 12 weeks or longer. Consequently, with a waiting period like 90 days, the family can expect to pay out of pocket for care for five to six -plus months prior to receiving a payment from the insurer.
Note: Sometimes families hold invoices until the claim decision is finalized. But they should submit them right away so they can be paid when the claim is approved. In fact, one can contact the insurer even before they receive an invoice—like to obtain provider approval. (Typically, the elimination or waiting period begins from the first date of qualified care service.
Setting proper expectations can avoid turmoil and stress. Insurers need adequate documentation supporting the insured’s eligibility and plan of care. Unfortunately, the psychology of getting old is that insureds are likely to overstate their abilities at doctors’ appointments. They may conceal their declining physical or mental condition due to embarrassment and/or fear of losing their independence.
For example, during an assessment, one claimant denied problems with continence while he was literally wearing Depends. Insureds are inclined to talk about their best days but perhaps they should describe their worst too. Consider “sundowning” with dementia (confusion, agitation, pacing, aggression) which gets worse late in the afternoon or evening. Knowing this, should one schedule the cognitive assessment in the morning when they are at their best?
Unfortunately, sometimes doctors’ notes are written optimistically to protect patients’ feelings—thereby complicating benefit eligibility. Doctors today generally do not supply the same amount of detail they did years ago. They may click a digital option from a selection describing the patient’s condition vs. a personalized written narrative.
The family should review the insured’s medical records and encourage doctors to be forthcoming, detailed, and prompt. Additionally, consider that billing specialists are motivated to submit paperwork, so doctors get paid—whereas LTC claims requests may be a lower priority.
The insured/families are responsible for assembling records from physicians and caregivers and submitting them to the insurer. Insurers have very specific criteria (fax, mail, portal, email) which seniors may find challenging.
Important: while insureds are known to overstate their abilities—sometimes they or their families exaggerate or misrepresent their condition. This confuses and delays benefit eligibility. Therefore, be up-front and honest—since insurers may elect to engage an investigator for questionable claims.
Manage Expectations—Your Engagement Your clients should read their LTCi policy. Afterwards, they should read it again. Reviewing the contract, obtaining medical and care provider records along with communicating with the insurer is an arduous task. Although well-intentioned, you likely won’t have the time or expertise to do this. So, don’t get in over your head and commit to assisting when you are unable to. However, you can arm clients with basic knowledge to help them manage the claim or refer them to a LTC claims consultant who will charge a fee for their professional services.
Let them know up-front if you will be engaged or not. The very last thing you want to do is antagonize them. Appropriately managing expectations can leave a good impression on your clients and their family.
Client Considerations
Do Not let the policy lapse.
Urge families to sign up for third party notification to prevent lapses.
If the policy has lapsed due to cognitive impairment or functional incapacity, quickly explore if the policy can be reinstated.
Review coverage parameters. Get a copy of the policy if necessary.
Did the client make a change to reduce their benefits such as during a rate increase or otherwise?
Encourage families to select one point person to interact with the insurer.
Consider setting up Power of Attorney (POA). Obtain necessary paperwork like HIPAA release forms to allow the insurer to communicate with physicians and caregivers.
Ask about the insurer’s claims process. Find out how providers are assessed and get suggestions about care coordinators. Ask about discounts for LTC services.
Ensure the trusted family member/POA is present each time the insured interacts with the insurer.
Seniors on their own may get confused and not disclose sensitive care needs which harms their eligibility for benefits.
Be prepared to supply the following (a) a copy of the license for the home health care provider or facility (b) the health care practitioners Plan of Care (c) the care provider’s daily caregiving notes (d) invoices for care services and (e) a list of the physicians and medications.
Policy Provisions to Review
What criteria trigger benefit eligibility?
How long is the Waiting/Elimination Period? How exactly is it counted?
What is the Maximum Daily/Monthly Benefit?
Will the maximum benefit increase annually?
What Is the Lifetime Maximum Benefit Amount?
What types of care services are covered and how are they defined?
Does the Benefit Amount, Elimination Period, or Benefit Period vary for Home Health Care v. Assisted Living Facility v. Nursing Home?
Is the policy Reimbursement (most common) or Indemnity?
Is there Joint coverage?
What riders are included in the policy?
Is there Waiver of Premium and when does it begin?
What exclusions apply?
If you want to learn more about LTC definitions you can refer to CLTC: A_Guide_For_Your_LTC_Insurance_Policy.pdf (certitrek.com)
Good News—Silver Lining While LTCi often gets a bad rap as having an onerous claims process, we should recognize insurers have the responsibility to avoid paying ineligible claims. They need adequate documentation to justify payment. The more prepared your clients are, the more pleasant their claims experience will be.
It’s human nature when we receive good service, like 10 times in a row, that we simply carry on silently. But if on the 11th visit, we have a bad experience, then it’s the one time we talk about. Now imagine if you have a negative experience with a claim while under the pain and duress of a loved one’s decline. It is magnified—unbelievably so.
We’ve all heard of heart-breaking LTC claims examples. But, in 2023 alone, $14+ billion of traditional LTCi claims were paid. We don’t hear enough about these heart-warming testimonials where they were rescued by their policy. Not just the insured, but their spouses and children too—who now can spend more quality time with them vs. caregiving. Perhaps it’s our own fault, as an industry. We fail to toot our own horn, particularly in November, during Long-Term Care Awareness Month.
In the U.S., there are over 10,000 people turning 65 every day. It’s been dubbed the silver tsunami. So, get ready. More and more of your clients will be contacting you about their LTCi policy. Be prepared to push the brakes and stop. Congratulate them on their purchase. Help manage expectations. Arm them with the knowledge that it will likely be a lengthy process—but to hang on and be patient. Then outline your ability to assist (or not), provide pointers to review their policy, or refer them to a third party.
The good news is, claim time is the time when the insurer delivers on their promise and it’s the time for you to serve the next generation, potentially your future clients.
The 2024 Milliman Long Term Care Insurance Survey, published in the July/August issue of Broker World magazine, was the 26th consecutive annual review of long-term care insurance (LTCI) published by Broker World magazine. It analyzed product sales, reported sales distributions, and detailed insurer and product characteristics.
From 2006-2009, Broker World magazine published separate group LTCI surveys, but discontinued those surveys when the availability of group LTCI policies shrank. In 2011, Broker World magazine began this annual analysis of worksite (“WS”) sales to complement the overall market analysis.
The WS market consists of individual policies and group certificates (“policies” comprise both henceforth) sold with employer support, such as permitting on-site solicitation and/or payroll deduction. If a business owner buys a policy for herself and pays for it through her business, participants likely would not report her policy as a WS policy because it was not part of a WS group. If an employer sponsors LTC/LTCI educational meetings, with employees pursuing interest in LTCI off-site, sales would likely not be reported as WS sales.
We limit our analysis to US sales and exclude “combination” products, except where specifically indicated. (Combination products pay meaningful life insurance, annuity, or disability income benefits in addition to LTCI.)
The bulk of worksite sales that cover activities of daily living (ADLs) or cognitive impairment do not qualify as LTCI under section 7702(B) and are not covered in this survey (except as specifically mentioned).
In addition to “WS” to represent worksite sales, we use “NWS” to represent individual (non-worksite) sales and “Total” to refer to WS and NWS sales combined.
About the Survey Participants: Seven insurers (Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian Life, New York Life, Northwestern, and Thrivent, referred to as “Participants” herein) contribute broadly to stand-alone sales distributions reported herein. Total 2023 sales data includes one additional contributor (LifeSecure) and 2023 inforce data includes two additional contributors (LifeSecure and CalPERS).
Our stand-alone LTCI WS sales and statistical distributions come from participants National Guardian Life, New York Life, and Northwestern; WS sales data from contributor LifeSecure; and inforce business from those insurers plus Mutual of Omaha.
The following ten insurers participated in our combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual (Northwestern), OneAmerica, Securian, Trustmark and United of Omaha.
Comparisons of sales distributions: WS statistical distributions can vary significantly from year-to-year if particular segments of the WS market are over- or under-represented (the three segments are core, carve-out, and voluntary, described later). Carriers that provided our 2023 distributions had an average worksite annual premium of $2,271, excluding FPOs and single premium policies, whereas insurers that provided sales, but not distributions, had an average annual worksite premium of $1,476. That discrepancy, consistent with the past several years, suggests that our worksite sales distributions are dominated by carve-out executive sales.
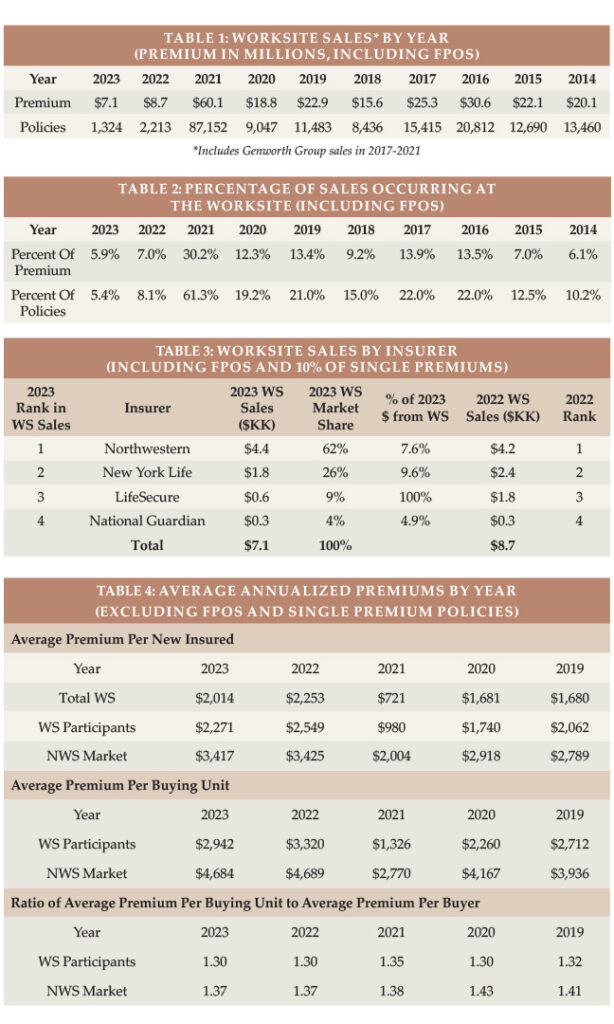
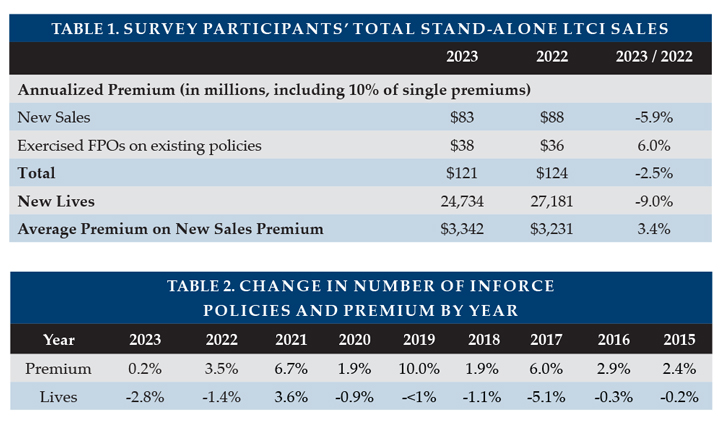
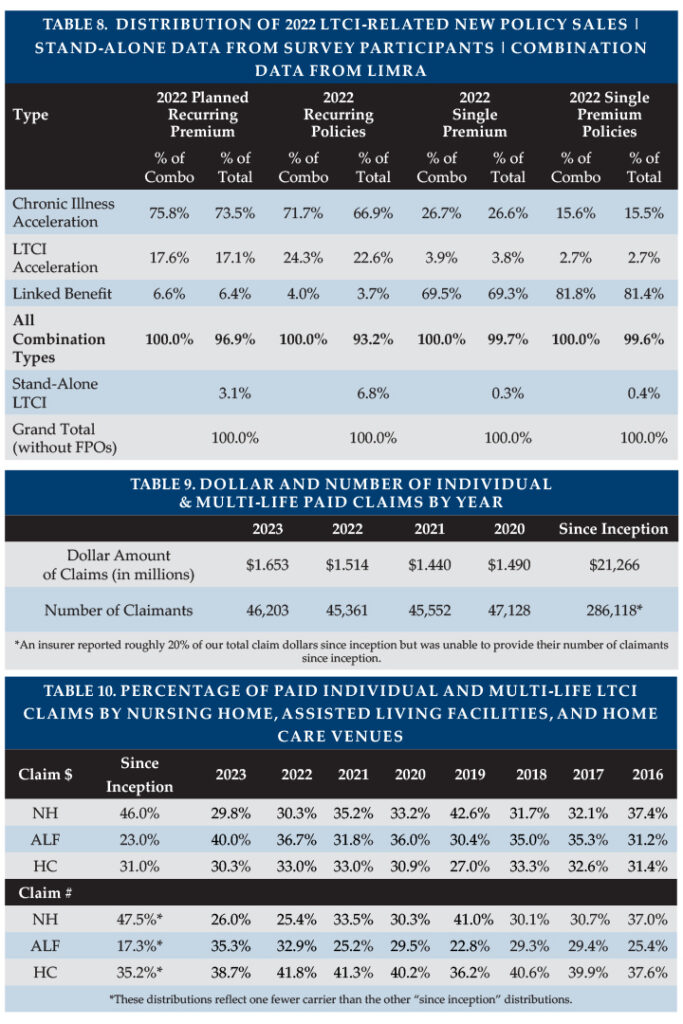
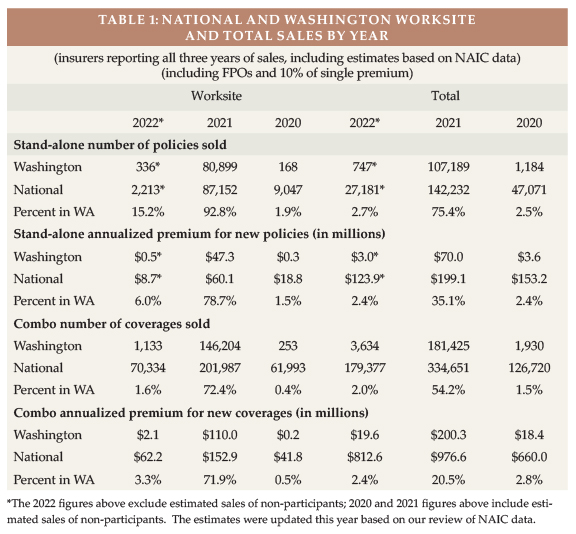
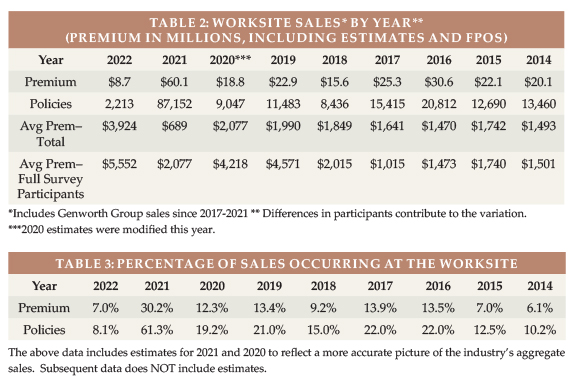
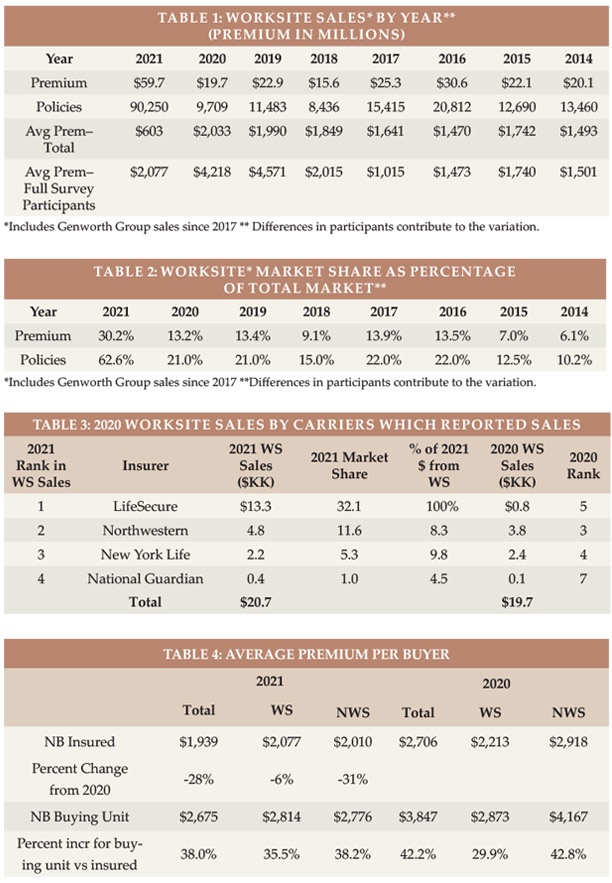
Highlights from This Year’s Survey Table 1 shows WS new sales by year (for 2023: 1,324 lives, down 40 percent from 2022, and $7.1 million of annualized premium, including FPOs, down 18 percent) and Table 2 shows the percentage of Total sales that were made in the WS by year (5.4 percent of lives and 5.9 percent of premium in 2023). The WS stand-alone LTCI market has reduced substantially since the major writer discontinued sales in 2021 and is a decreasing percentage of the Total market. As discussed previously, some sales that are worksite-related may not be classified as WS sales.
Over at least a 20-year period prior to 2022, the fewest stand-alone worksite LTCI policies sold in a year was 8,436 policies (2018). Worksite sales with coverage for ADL-deficiency and cognitive impairment have shifted to combination policies, most of which do not qualify as LTCI under section 7702(B). Only two of the carriers in that market reported combo worksite sales for our survey, but those two carriers sold roughly 80,000 such worksite policies in 2023 (up 16 percent from 2022) compared to the industry’s 1,324 stand-alone LTCI WS sales. Among our combination contributors, WS sales accounted for 36.3 percent of reported lives and 9.9 percent of annualized premium. We have a good-sized sample of combination insurers, but a lower percentage of industry sales than in the stand-alone market.
MARKET PERSPECTIVE There are three segments of the WS market. A single WS case may involve different segments for different employee classes.
In “core” (“core/buy-up”) programs, employers pay for a small amount of coverage for generally a large number of employees. Employees can buy more coverage. “Core” programs generally have low average ages, short benefit periods, low daily maximum benefits and a small percentage of spouses insured.
In “carve-out” programs, employers pay for robust coverage for key executives and usually their spouses. Generally, executives can buy more coverage for themselves or spouses. Compared to “core” programs, a higher percentage of insureds are married and more spouses buy coverage. Because the age distribution is older, the maximum monthly benefit is higher, and the benefit period is longer, the average premium is much higher than for core programs.
In “voluntary” programs, employers pay none of the cost. The typical coverage is more robust than “core” programs, but less robust than “carve-out” programs. Voluntary programs tend to be most weighted toward female purchasers.
Because of tax savings, small executive carve-out issue dates may have effective dates weighted toward the end of the year. On the other hand, large voluntary cases are more likely to have fall enrollments with January 1 effective dates.
National Guardian, New York Life, and Northwestern write mostly executive carve-out programs and are the only insurers that provided statistical worksite distributions; therefore, our distributions are heavily weighted to the executive carve-out market.
Carrier and product shift: Voluntary WS programs have gravitated toward combination products that include life insurance because insurers, brokers, employers, and employees tend to favor combination products.
Insurers’ pricing, underwriting, and distribution considerations favor combination products. Prior to 2012, insurers used unisex “street” pricing and typically discounted “street” prices by five percent for the worksite. Gender-distinct “street” pricing made WS pricing more complicated for insurers who believe unisex pricing is preferable in the WS due to Title VII of the 1964 Civil Rights Act. Pricing, state filing, administration, and illustration work increased when insurers could no longer simply reduce “street” prices by five percent.
Because women have higher expected future claims, unisex pricing saves women money compared to gender-distinct NWS pricing. On the other hand, men pay much more (e.g., roughly 50 percent more for some insurers) with unisex pricing than with gender-distinct pricing, possibly complicating WS sales and raising insurer concerns about gender anti-selection (a higher percentage of females in WS cases). Insurers also fear health anti-selection (unhealthy people being over-represented among buyers), as stand-alone LTCI does not have a high voluntary participation rate. Therefore, WS stand-alone LTCI programs have limited, if any, underwriting (health) concessions.
Combination products with LTC-related benefits are less affected by unisex pricing as females pay less for the death benefit but more for the LTCI (or chronic illness) benefit. Furthermore, products with chronic illness riders do not require salespeople to be LTCI-certified, which provides insurers access to a broader distribution system than with stand-alone LTCI. As combination life programs have higher penetration rates, insurers often offer “guaranteed issue,” coverage based on the number of employees and participation rates.
From the broker, employer, and employee perspective, simplicity is very attractive. “Guaranteed issue,” along with typically fewer age restrictions than for unisex stand-alone LTCI pricing, allows any employee to be covered and makes enrollment easier and faster, like other employee benefit offerings.
Additionally, combination products’ death benefit avoids the “use it or lose it” issue and is more meaningful for young and less affluent people than is LTCI. Such products can allow 100 to 300 percent of the death benefit to be used for help with ADLs or cognitive impairment, typically using up to four percent of the death benefit each month. Alternatively, they can allow 100 to 200 percent of the death benefit (at a rate of four percent per month) but restore the death benefit each month when a LTCI claim is processed. With “restoration”, beneficiaries will receive the full death benefit regardless of how much LTCI benefit was received. Most of these provisions qualify as “chronic illness” under IRS §101(g); others qualify as “long-term care insurance” under IRS §7702(B). The chronic illness products do not require broker LTCI certification, which makes those products “simpler” than §7702(B) products.
While stand-alone (and linked-benefit) individual LTCI products generally offer annually-increasing coverage to try to maintain purchasing power in the face of inflationary increases in the costs to provide long-term care, WS combination products have a fixed benefit. For example, if a 30-year-old employee buys a $100,000 death benefit, she will have a $4,000 monthly benefit for chronic illness (assuming the benefit features described above). That $4,000 benefit would have much more purchasing power if she needs care in the next few years than if she needs care 50 years from now.
Stand-alone LTCI is still popular in executive carve-out programs. Executives can more easily afford to continue coverage after termination of employment, hence appreciate the value of compound benefit increases. Income tax advantages encourage employer-paid coverage, particularly for executives, and tax advantages may increase in the future if income tax rates rise or if such LTCI coverage permits opting out of future state LTCI programs. Because of tax advantages and employer premium payment, higher unisex prices for men are less of an issue in the executive carve-out market. Two stand-alone LTCI insurers offer unisex pricing with as few as 2 to 5 (varies by jurisdiction) employees buying, an approach that caters to this market.
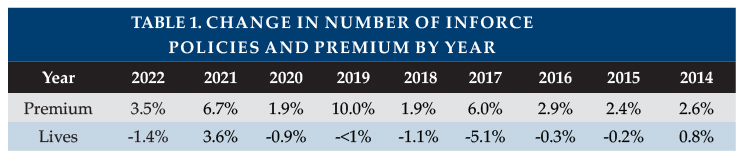
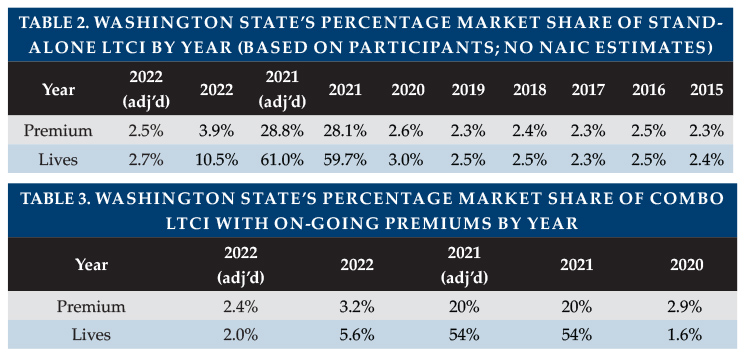
State-run LTCI programs: We discussed state-run LTCI programs in the July/August issue and prior years’ articles. Washington state’s “Washington Cares Fund” (WCF) stimulated tremendous market demand in the state of Washington, causing WS sales and distributions to vary greatly from historical trends in 2021 and 2022. However, the Washington Cares Fund and other potential state-run programs appear to have had little impact on 2023 WS sales.
Availability of coverage: As few people younger than age 40 buy stand-alone LTCI, some insurers have raised their minimum issue age to avoid anti-selection and to reduce exposure to extremely long claims. One insurer limits the maximum age to 69. Such age restrictions can discourage employers from introducing a program (even a carve-out program if they have executives or spouses too young to be covered).
Younger employees who are ineligible for coverage may still benefit from a program because their elders are often eligible for WS stand-alone LTCI programs. However, one contributor no longer offers WS LTCI to non-household relatives. Reduced availability for such relatives does not have much impact on sales, because typically 99 percent of worksite sales are to employees or their partners. Thus, even if a program is available to elder relatives, it is not likely to meaningfully address the negative impact of employees being caregivers.
With increased remote work, more employers have employees stretched across multiple jurisdictions. Eligible non-household relatives might live anywhere. However, insurers may not offer a product in jurisdictions with difficult laws, regulations, or practices, such as slow policy form approval. It can be hard to find a product which can cover everyone unless LTCI is sold on a group policy form and the employer does not have individuals in extra-territorial states. Combination products also run into jurisdictional issues because some jurisdictions do not allow LTCI benefits to exceed the death benefit and/or do not allow death benefit restoration.
Increasing hurdles for coverage have discouraged brokers as well as insurers. Some employee benefit brokers are reluctant to embrace stand-alone LTCI because of declinations, the enrollment effort compared to typical group coverages, certification requirements, their personal lack of expertise, etc. These issues could be mitigated by LTCI specialists forming relationships with employee benefit brokers.
Support for Employees who are Caregivers: Various programs offer LTC-related services to employees and their families. Regardless of whether the employee is insured or the relative is insurable, they may be able to access information, advice, services, and products that make caregiving more efficient, more effective, safer, and less expensive. Enabling employees and their families to have better LTC experiences and to use more (not necessarily 100 percent) commercial care should boost productivity at work. Some of these programs are packaged with WS LTCI.
STATISTICAL ANALYSIS In addition to fundamental industry changes, distributions may vary significantly from year to year due to different participants, shifting distribution within an insurer, and changing market share among insurers. Our sales distributions reflect only stand-alone LTCI. Two insurers reported their number of new employer cases as well as the number of new worksite sales. Combined, they averaged 5 applications per new employer case, which seems to confirm the executive carve-out concentration in our data.
Aggregate Sales Table 1 shows the number of sales and premium in the worksite market by year. As noted above, the worksite market is in decline, with the exception of 2021 due to sales stimulated by the WCF. The shrinkage of the stand-alone WS market is underscored when you consider that nearly two-thirds of 2023 WS premiums came from FPOs on past years’ sales.
Table 2 shows WS sales as a percentage of total LTCI sales. As the market shrinks, the impact of FPOs on past sales becomes larger. FPOs account for WS being a higher percentage of premium (5.9 percent) than policies (5.4 percent). Removing FPOs, the WS premium is 3.2 percent of the total. The 2022 percentages are slightly inflated due to runout sales in Washington.
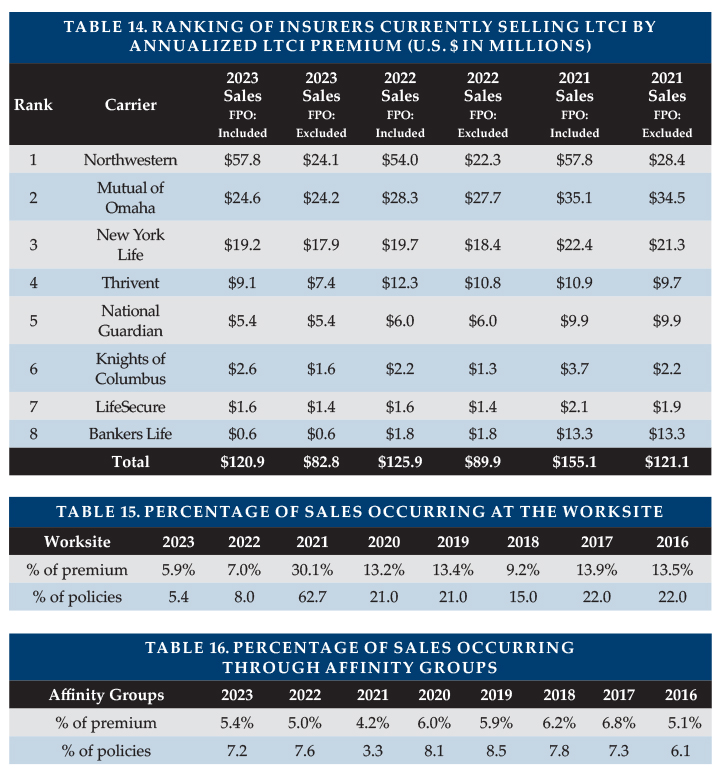
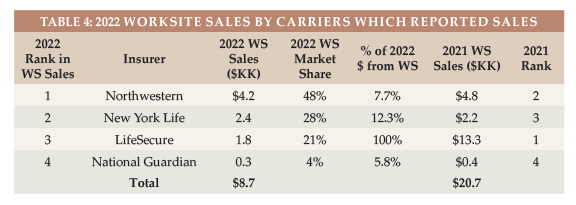
Market Share Table 3 shows the insurers’ reported WS sales, including FPOs and new sales to worksite cases issued in prior years. Excluding FPOs, New York Life would have been in the lead, followed by LifeSecure.
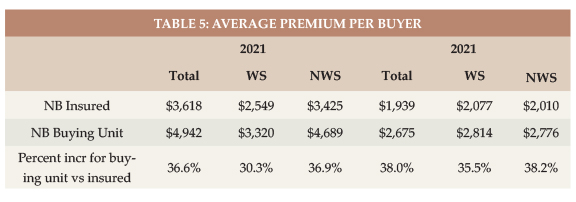
Average Premium Per Buyer Table 4 shows the average premium (without FPOs and without single premiums) per new insured for WS contributors, for WS participants (insurers which provided distributions), and for the NWS market. The total WS market has a lower average premium than those WS carriers that provided distributions. When comparing the WS market to the NWS market, influences such a younger average issue age drive the lower WS average premium.
Table 4 also shows the average premium per buying unit for insurers that provided distributions (a couple comprise a single buying unit). The average premium per buying unit is higher because there are fewer buying units than insureds. The ratio between average premium per buying unit and average premium per insured life is consistently lower for WS sales, because more WS buyers are single and because spouses are less likely to buy in the WS. However, Table 4 likely understates the difference because our WS distributions reflect a higher concentration from the carveout market, which has a lot of couples who both buy.
Issue Age In reviewing the balance of the statistical presentations, we urge you to be selective in how you use the data because it is not representative of the entire WS market as explained above.
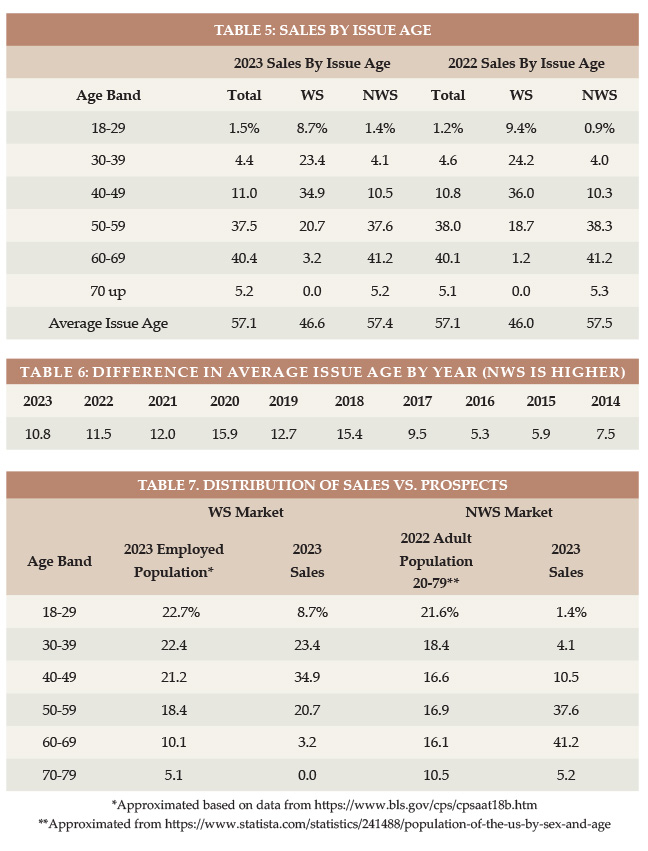
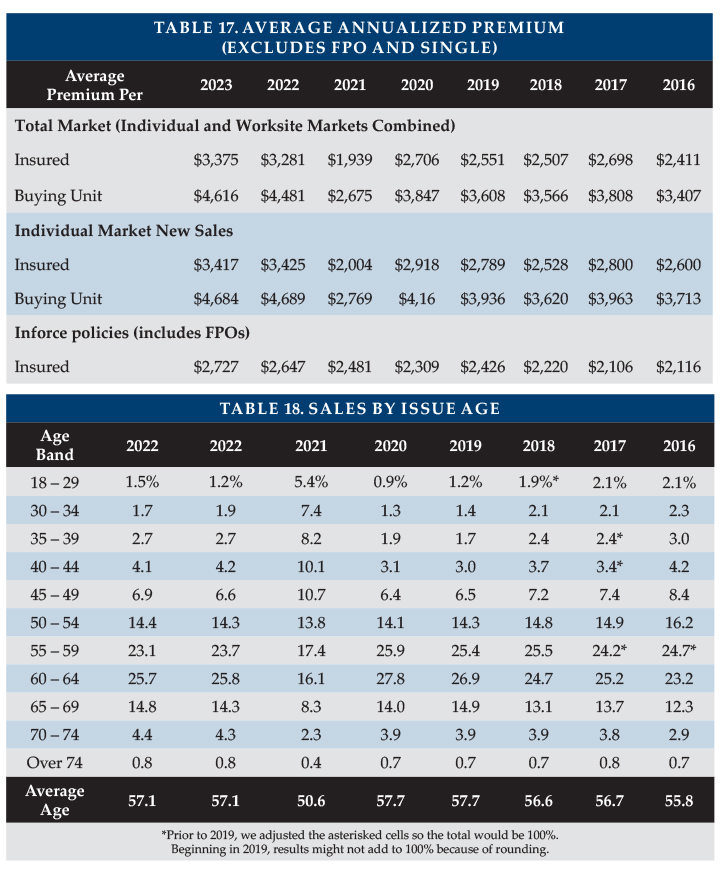
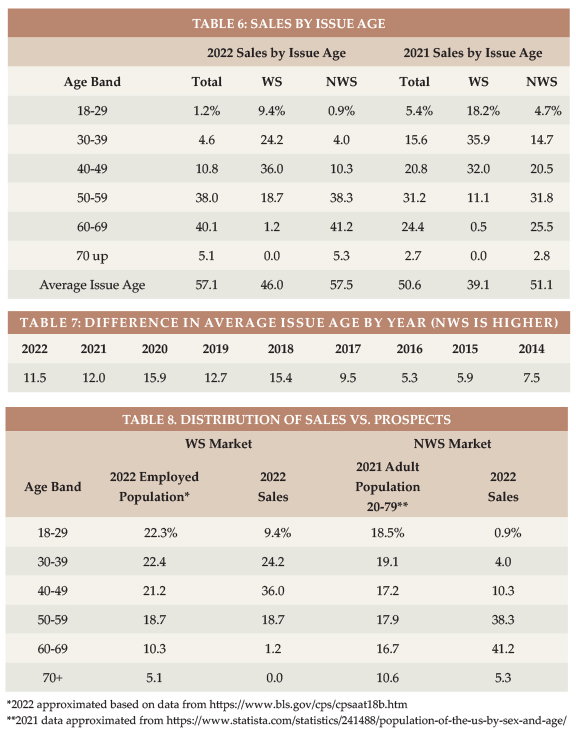
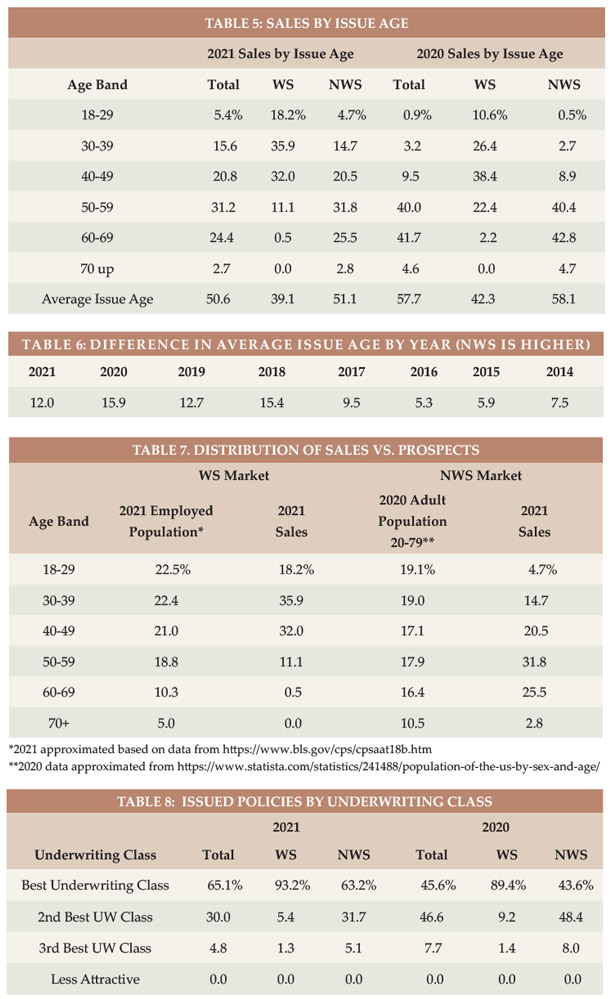
Table 5 shows the distributions by issue age and Table 6 shows, by year, how much older the average age NWS buyer is than the average age WS buyer.
Table 7 displays the relative age distribution of workers ages 18+ compared to the age distribution of purchasers in the WS market and the age distribution of adults 20-79 compared to the age distribution of purchasers in the NWS market. If the percentage of sales in a particular age group is higher than the percentage of population in that age group, we can conclude that LTCI is more appealing to that age group, the industry gets in front of that age group more, and/or more of the applicants in that age group qualify for coverage. In the WS market, the industry is particularly effective with ages 40-49. In the NWS market, the industry is particularly effective for ages 50-69.
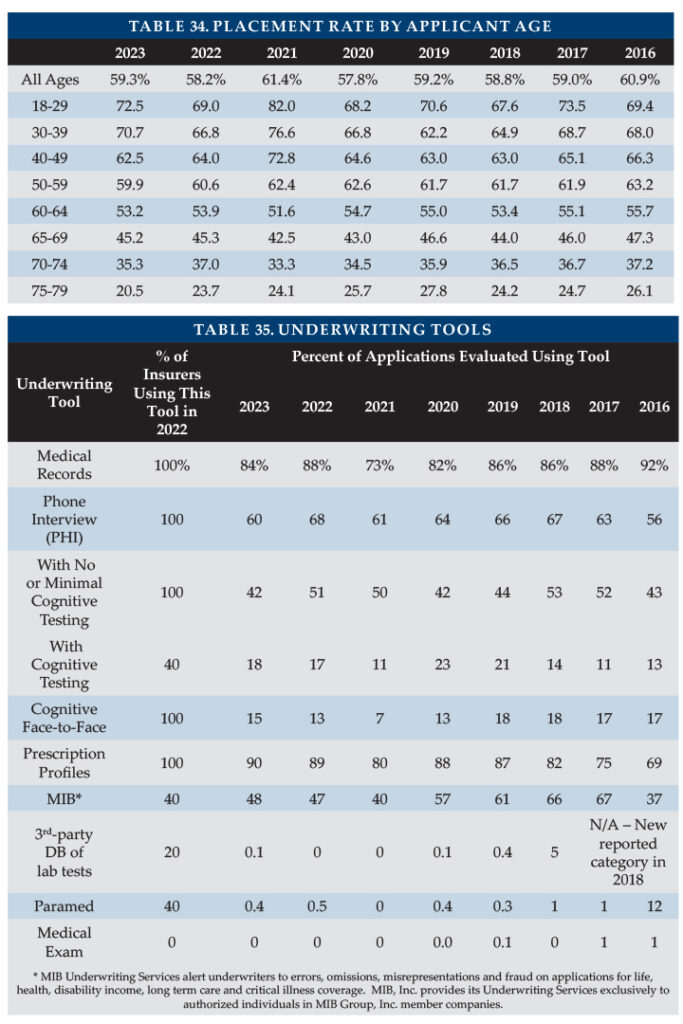
Rating Classification Three of our seven contributors do not offer a “preferred health” discount, so the bulk of their sales are in their best underwriting class. They are also the insurers providing WS distributions, which contributes to the high percentage (92 percent) of worksite policies issued in the best underwriting class, as shown in Table 8.
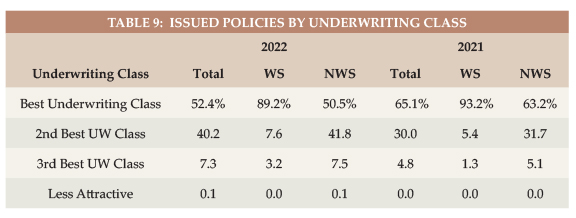
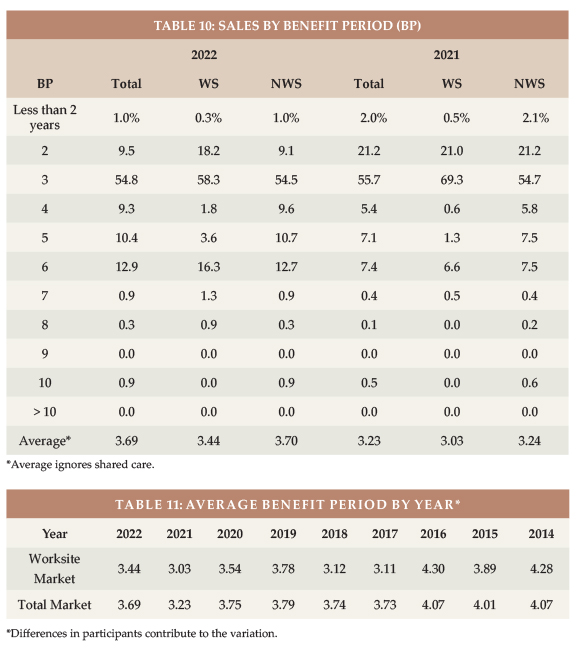
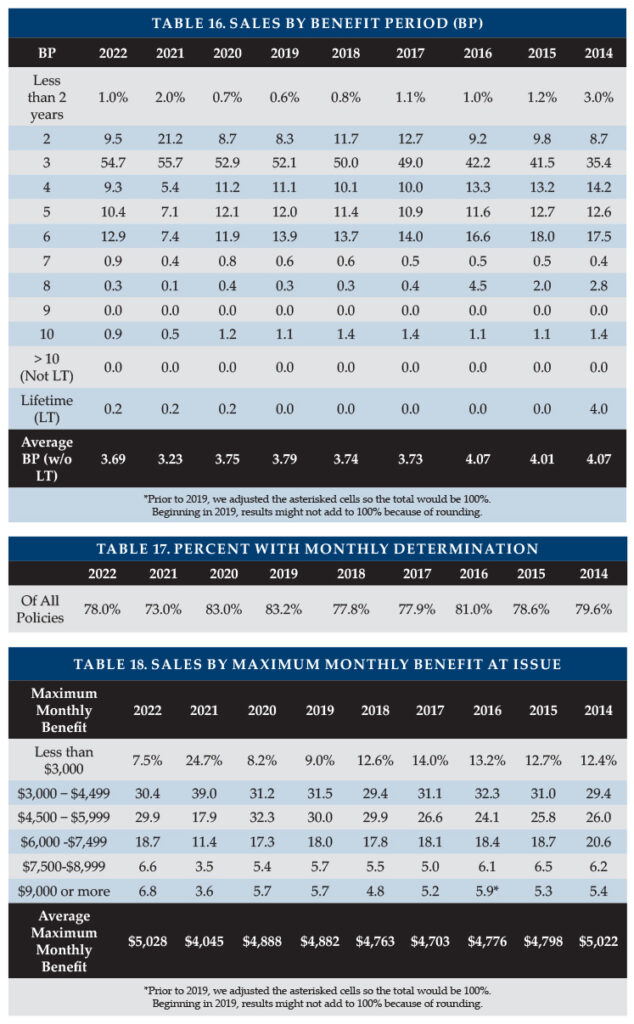
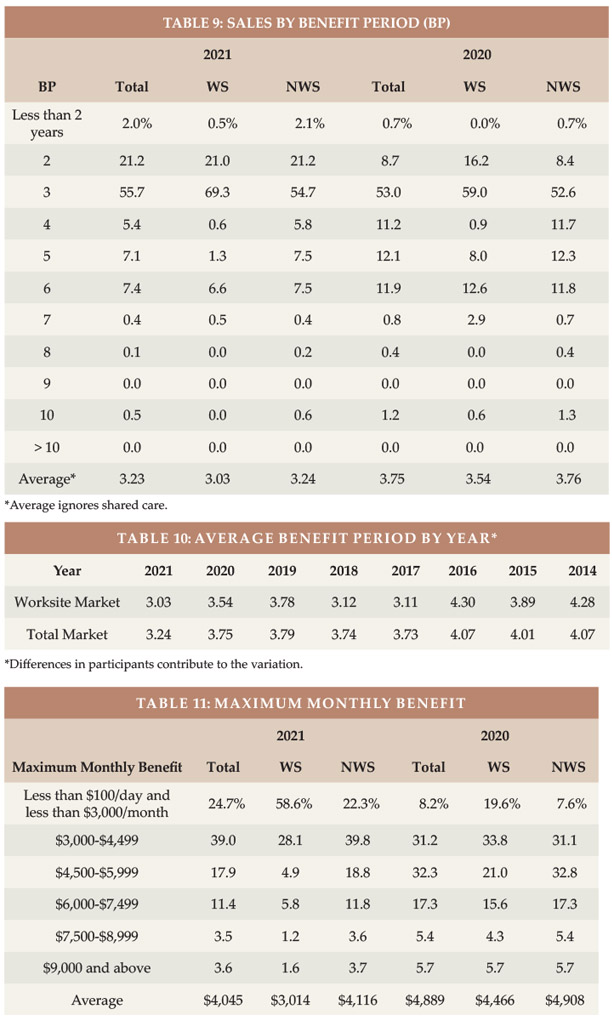
Benefit Period The WS average benefit period is low for core/buy-up programs and somewhat low for voluntary programs. Executive carve-out programs sometimes have longer benefit periods than the NWS market. In 2023, the WS market, for the first time since 2016, had a slightly longer average benefit period than the total market (see Table 9). Table 10 shows the results by year. Note that these statistics ignore Shared Care which, in effect, lengthens benefit period and is more prevalent in the NWS market.
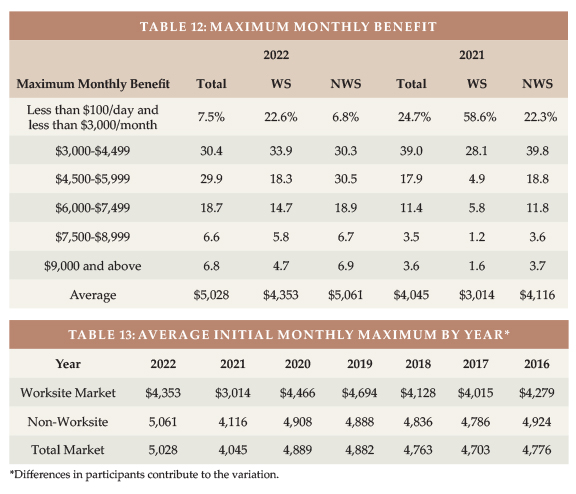
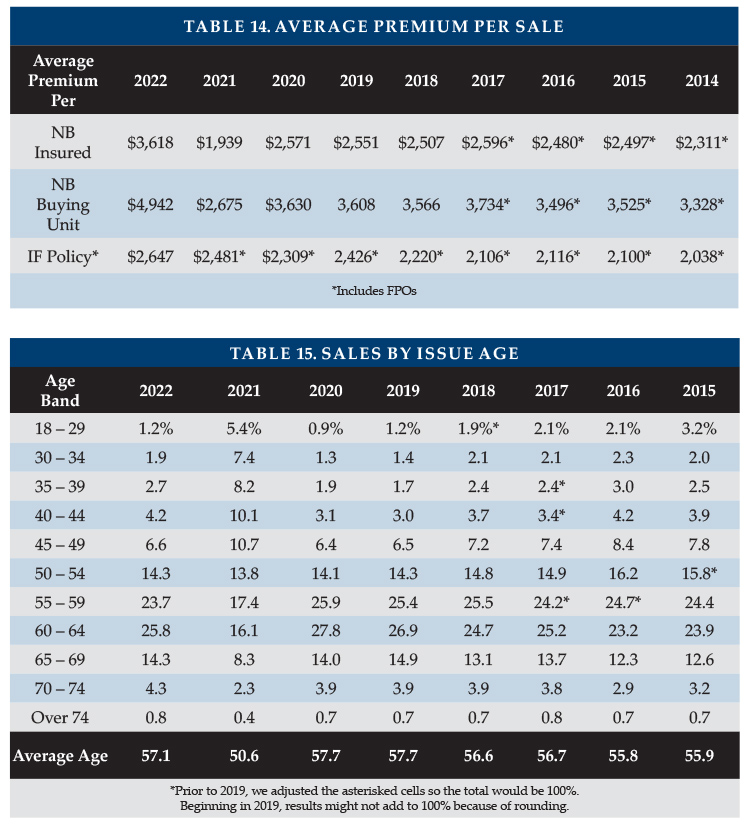
Maximum Monthly Benefit To calculate the average initial monthly maximum, we presume an average size in each size range shown in Table 11. While the WS market had a slightly longer average benefit period in 2023 than did the NWS market, it had a smaller average initial monthly maximum. Table 12 shows that the initial maximum monthly benefit hit record high levels in 2023. The WS initial monthly maximum varies more over time than the total market because of participant changes and how many core/buy-up plans were sold in a particular year.
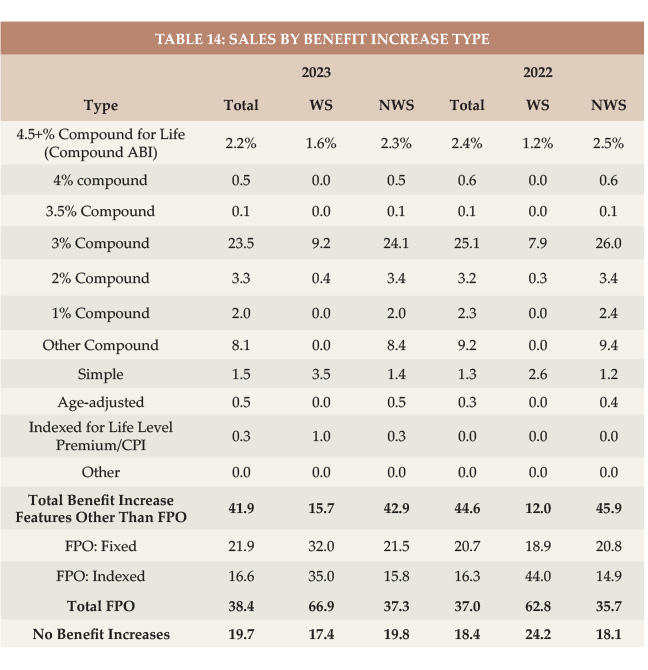
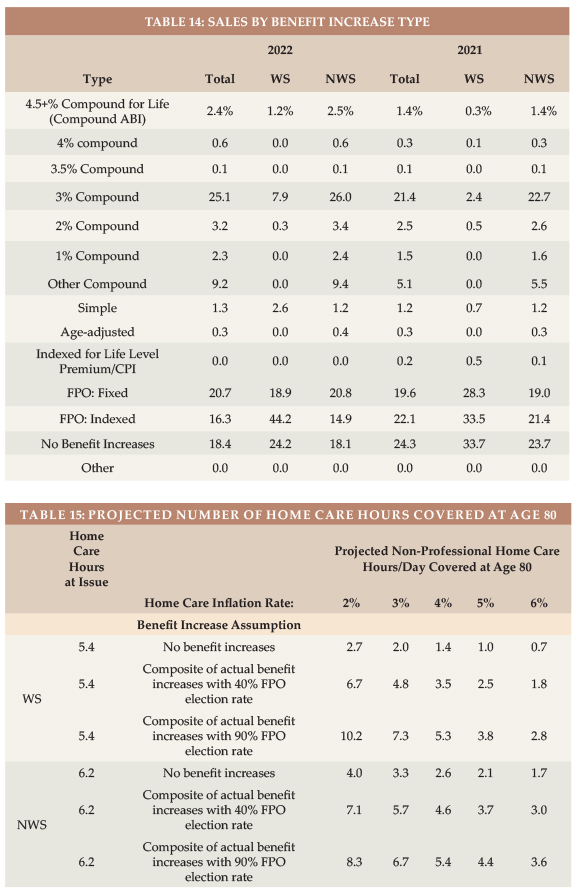
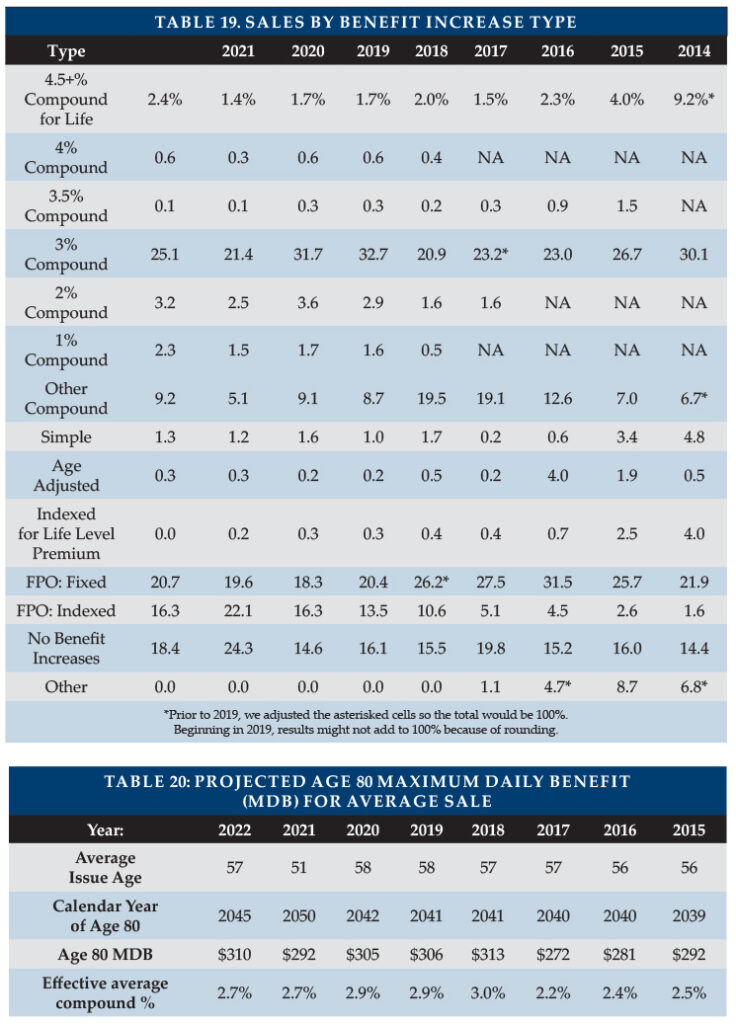
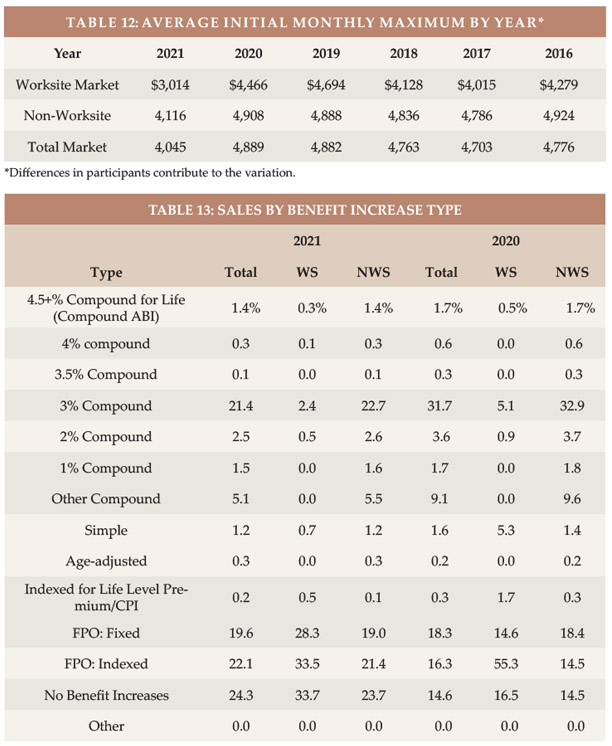
Benefit Increase Features As shown in Table 14, 10.8 percent of 2023 WS sales had compounding of three percent or higher, compared to 9.1 percent in 2022. Of the 2023 WS sales, 17.4 percent had no increase feature and 67 percent had a FPO feature.
In the NWS market, 26.9 percent had three percent or higher compounding compared to 29.2 percent in 2022. While three percent or more compounding is dropping in the NWS, it is increasing in the WS market, albeit still much less common in the WS market.
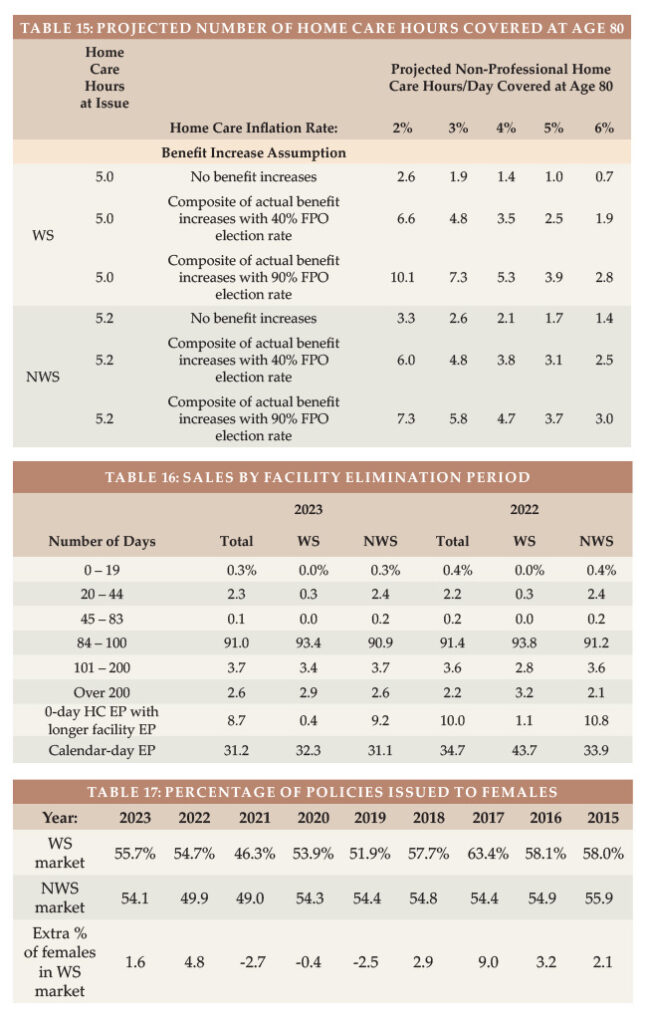
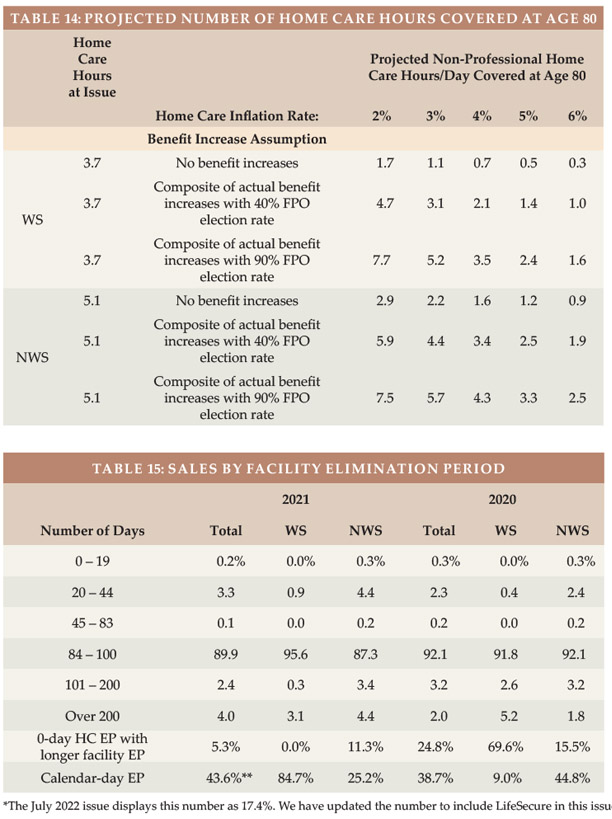
Future Protection Based on a $33/hour cost for home health aides (the median cost according to Genworth’s 2023 Cost of Care Survey), the average WS initial maximum daily benefit of $166 would cover 5.0 hours of such care per day at issue, whereas the typical NWS initial daily maximum of $173 would cover 5.2 hours of such care per day, as shown in Table 15.
The number of future home care hours that could be covered depends upon when care is needed (we have assumed age 80), the home care cost inflation rate between now (age 47 for WS and 57 for NWS) and age 80 (we have calculated with 2, 3, 4, 5 and 6 percent inflation), and the benefit increases provided by the LTCI coverage between now and age 80.
Table 15 shows calculations for three different assumptions relative to benefit increase features:
The first line presumes that no benefit increases occur (either sold
without any benefit increase feature or no FPOs were exercised).
The second line reflects the average benefit increase design using the methodology reported in the July/August article, except it assumes that 40 percent of FPOs are elected (intended to be indicative of “positive” election FPOs, in which the increase occurs only if the client elects it) and provide five percent compounding.
The third line is like the second line except it assumes 90 percent of FPOs are elected (intended to be indicative of “negative” election FPOs, in which the increase occurs unless the client rejects it). It also assumes the FPOs reflect five percent compounding.
Table 15 indicates that:
Without benefit increases, purchasing power deteriorates significantly, particularly for the WS purchaser as younger buyers have more years of future inflation prior to claim onset. For example, with a flat benefit, the number of covered hours of home care at age 80 drops to 1.9 hours for the average WS purchase age if there is three percent inflation. The average NWS buyer would have 2.6 hours of care (rather than 1.9 hours) at age 80 if they had no benefit increases and inflation was three percent because the average NWS buyer is older (and secondarily, buys a larger daily benefit).
The “composite” (average) benefit increase design assuming that 40 percent of FPO offers are exercised preserves purchasing power better than when no increases are assumed. The average WS buyer gains buying power over time if the inflation rate is two percent, being able to pay for 6.6 hours at age 80. But if the inflation rate is four percent, this drops to 3.5. The average NWS buyer generally does better because of a higher issue age, more robust benefit increase features and a higher initial maximum daily benefit. However, the WS market has more FPOs, so when we assume 90 percent FPOs election, the WS market does better. It also does better with 40 percent FPO election and a two percent inflation rate because we presume a full five percent FPO will be exercised.
Assuming that 90 percent of FPO offers are exercised, the average WS buyer would have at least as much coverage at age 80 as at issue if the inflation rate is less than four percent. The average NWS buyer has increasing purchasing power unless inflation averages four percent.
Table 15 underscores the importance of considering future purchasing power when buying LTCI. Please note:
a) The average 2023 WS buyer was 10 years younger at issue than the average 2023 NWS buyer, hence has 10 more years of inflation and benefit increases in Table 15. The actual inflation rate to age 80 is not likely to be the same for today’s 47-year-olds as for today’s 57-year-olds.
b) Individual results vary significantly based on issue age, initial maximum monthly benefit, and benefit increase feature, as well as the inflation rate and the age at which the need for care occurs.
c) By the median age of starting to need care (about age 83) and the median age of needing care (about age 85), more purchasing power could be gained or lost.
d) Table 15 does not reflect coverage for professional home care or facility care. According to the 2023 Genworth study, the median nursing home private room cost is $320/day, which is currently comparable to 10 hours of non-professional home care. However, the inflation rate for facility costs is likely to differ from the inflation rate for home care. From 2004-2023, Genworth’s studies showed the following compound growth rates: private room in a nursing home (3.1 percent), assisted living facility (4.3 percent), home health aide (2.7 percent), and home care homemaker (3.1 percent).
e) Table 15 could be distorted by simplifications in our calculations. For example, we assumed that the FPO election rate does not vary by age, size of policy or market and that everyone buys a home care benefit equal to the average facility benefit.
Partnership Program Background When someone applies to Medicaid for long-term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (with some policies, IN and NY disregard all assets). Partnership programs exist in 44 jurisdictions (all but AK, DC, HI, MA, MS, UT, and VT), but MA has a similar program (MassHealth). The first four states to develop Partnerships (CA, CT, IN and NY) have different rules, some of which have become a hindrance to sales. We are not aware of a Partnership-qualified WS LTCI product in those four states, which is unfortunate because the WS market serves many people who could benefit from Partnership.
To qualify for a state Partnership program, a policy must have a sufficiently robust benefit increase feature. At least 29 jurisdictions have lowered the minimum Partnership-eligible compounding benefit inflation rate to one percent. To facilitate Partnership sales in such jurisdictions, an insurer could lower its minimum size from $1,500 to $1,000 if one percent compounding is included in a core program. The policies would qualify for the state Partnership and case revenue and core sales would likely increase. The premium would be more level by issue age, shifting risk to younger ages which can be preferable for the insurer in a core program.
Jurisdictional Distribution We also examined the market share (based on number of new insureds) by jurisdiction. As was the case last year, the WS market share of five states (AL, AK, HI, NC, & VT) was at least 50 percent higher than that state’s overall market share (e.g., if they had a two percent overall market share, they had at least a three percent market share in WS). This could be the result of a single large case in that state. In 18 jurisdictions (same number as last year), the market share of total sales was at least 50 percent greater than the WS market share, suggesting that there may be opportunity for WS sales in these jurisdictions: CO, DE, IN, KS, KY, LA, MA, MD, ME, MO, MS, NE, NH, NV, OR, RI, SD, and VA. (The 9 bold italicized states were in this list last year.) In 7 jurisdictions (up from 5), our participants had no stand-alone WS sales at all (DC, ID, NM, UT, WV, WY and Puerto Rico).
Click here for a chart of the market share of each US jurisdiction relative to the total, WS and NWS markets, and the Partnership percentage by state. This chart indicates where relative opportunity may exist to grow LTCI sales.
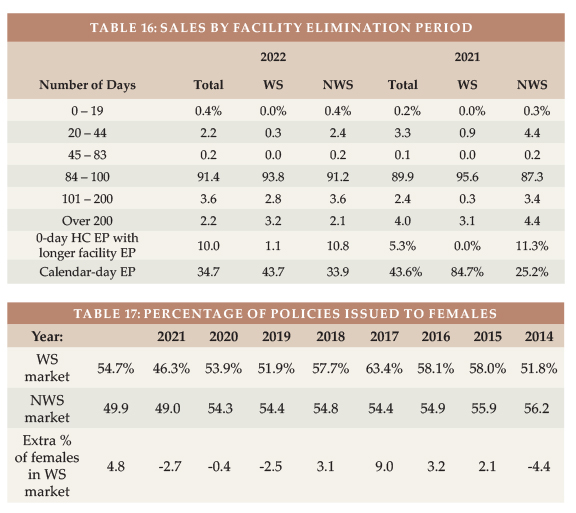
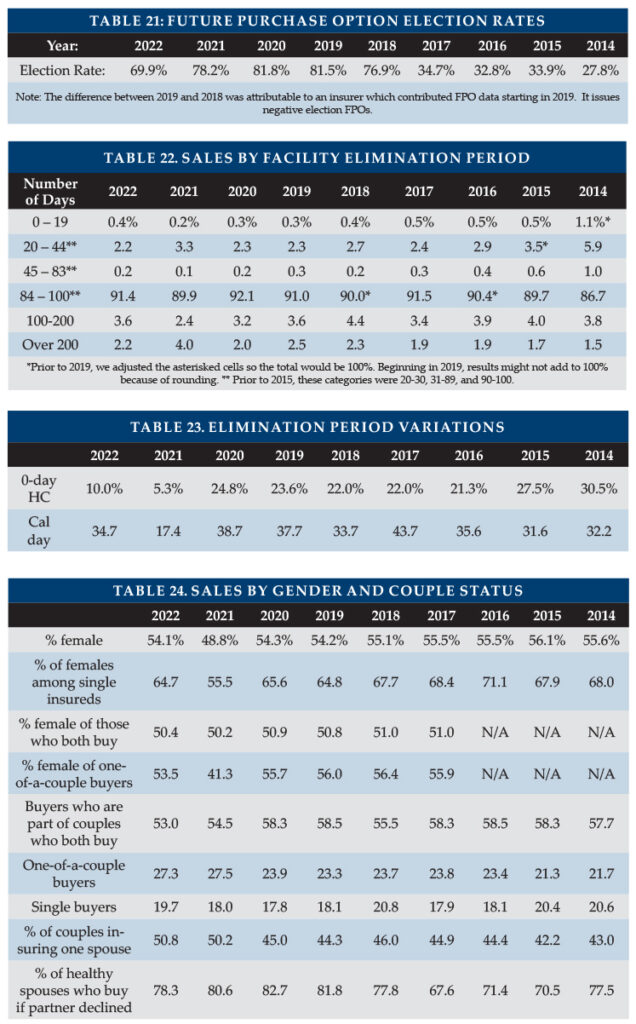
Elimination Period More than 90 percent of the NWS market buys 90-day elimination periods (EPs). For that reason, many WS programs offer only a 90-day EP.
Table 16 shows distribution by EP and how many policies had a 0-day home care feature and a longer facility EP and how many policies had a calendar-day EP (as opposed to a service-day EP). We have reflected that all LifeSecure policies are 90-day EP with a calendar-day definition. Policies which have 0-day home care EP and define their EP as a service-day EP operate almost identically to a calendar-day EP, because people in facilities get daily care.
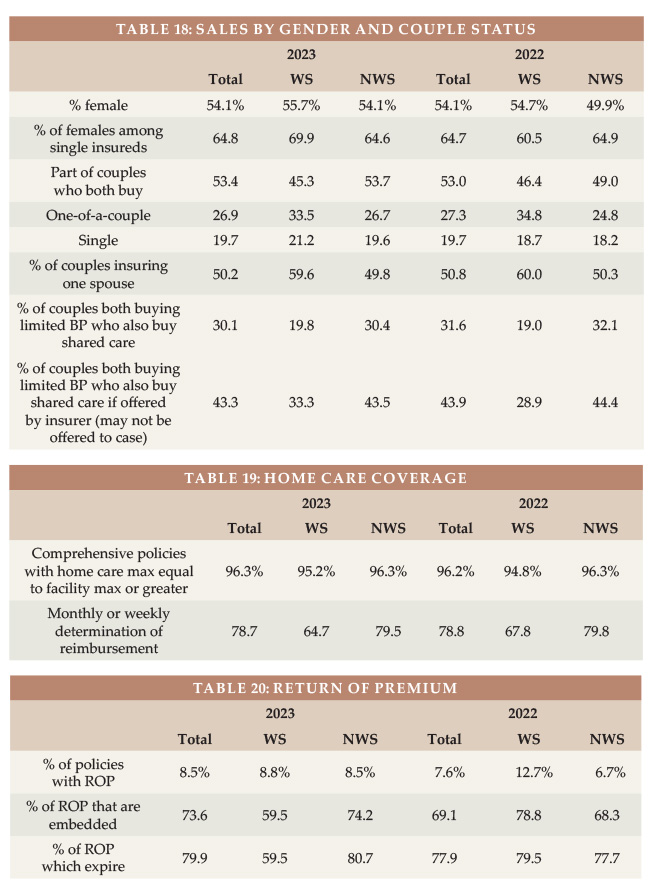
Gender Distribution and Sales to Couples and Relatives Insurers began gender-distinct LTCI pricing in 2013, but unisex pricing continues to be typical in the WS market because of Title VII of the 1964 Civil Rights Act.
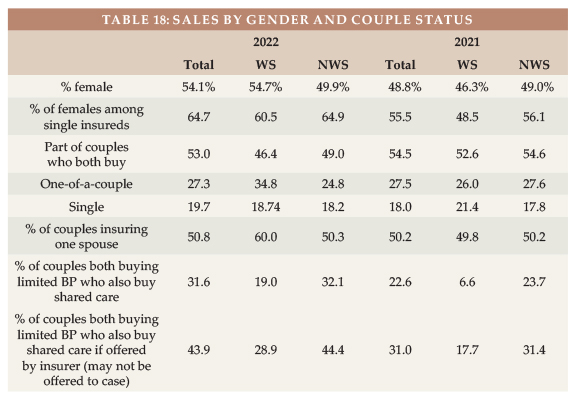
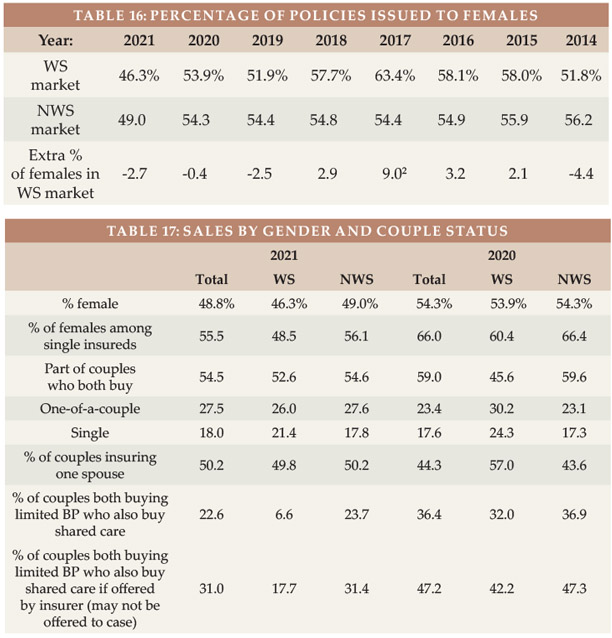
Women are 49.9 percent of the US age 20-79 population but have nearly always dominated LTCI sales1. Since 2016, the percentage of female buyers in the NWS has fluctuated from 54.1 to 54.9 percent (see Table 17), except for 2021 when the percentage of females dipped below 50 percent in both the WS and NWS markets because of the higher number of males purchasing coverage in WA. In 2022, the NWS market also had fewer than 50 percent females because of delayed processing of 2021 WA sales, but the Total market reverted to mostly female.
Table 17 also shows that the WS market generally experiences a higher percentage of female buyers (presumably because of unisex pricing), quantifying the above-mentioned “gender anti-selection” compared to the NWS market. To the degree that our WS data is over-weighted to executive carve-out programs, it likely understates the gender anti-selection of voluntary WS LTCI programs. Women make up 46.9 percent of workers but accounted for 55.7 percent of our reported 2023 WS sales2.
Table 18 digs deeper, exploring the differences between the WS and NWS markets in single female, couples, and Shared Care sales. Our WS data has more couples who insure only one partner (59.6 to 49.8 percent in the NWS market). Shared Care is less often offered in a WS program.
Our limited data with regard to relatives who buy shows that two spouses are insured for every three employees. That’s a high percentage reflective of executive carve-out data. Over time, we have seen about one percent of purchasers are relatives other than the employees and employees’ spouses.
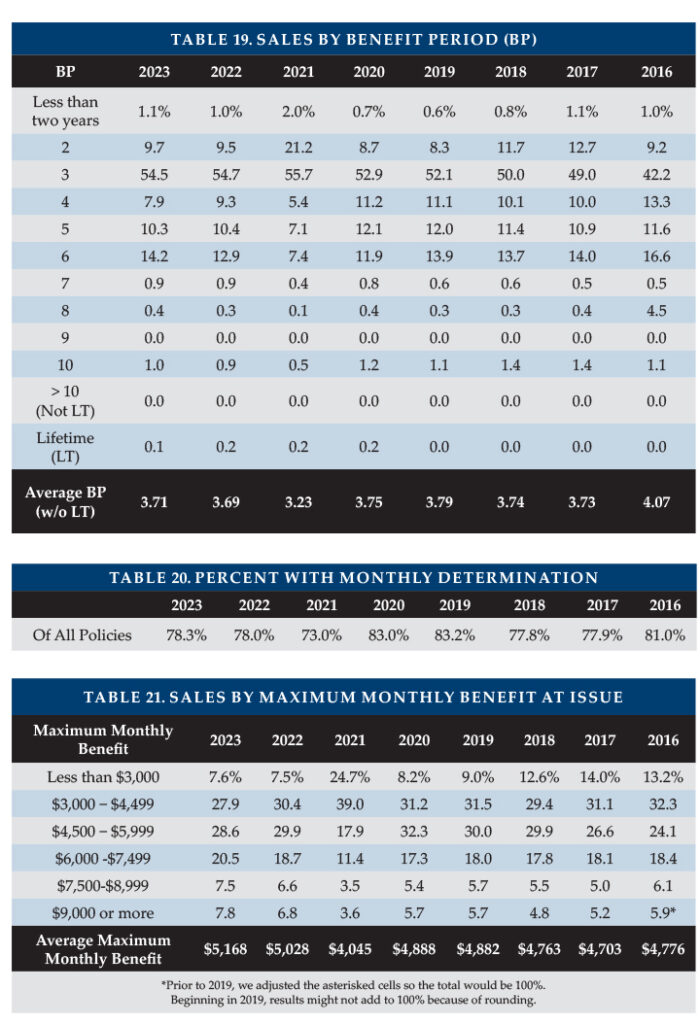
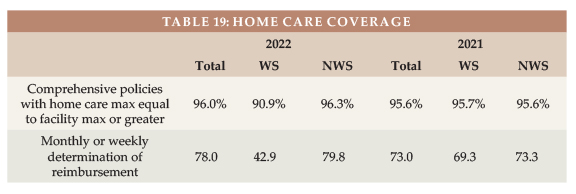
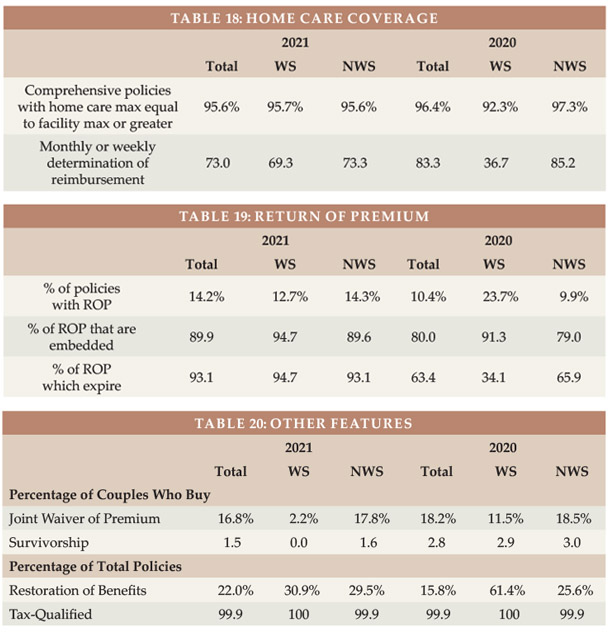
Type of Home Care Coverage Table 19 summarizes sales by type of home care coverage and shows the frequency of monthly determination of benefits. Long ago, WS policies’ home care maximum monthly benefits were 50 percent of the facility benefit; today they are generally identical.
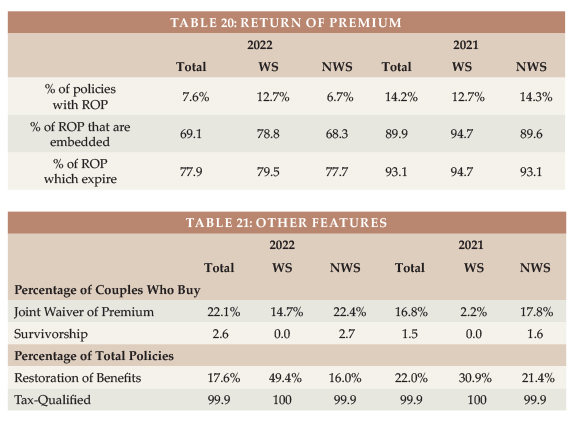
Other Features Table 20 shows that most Return of Premium (ROP) features are automatically included and phase out before death would be likely. ROP with expiring death benefits may provide an inexpensive way to encourage more young people to buy LTCI but does not address the buyer’s concern that they might pay all their life, then die in their 90s without qualifying for benefits.
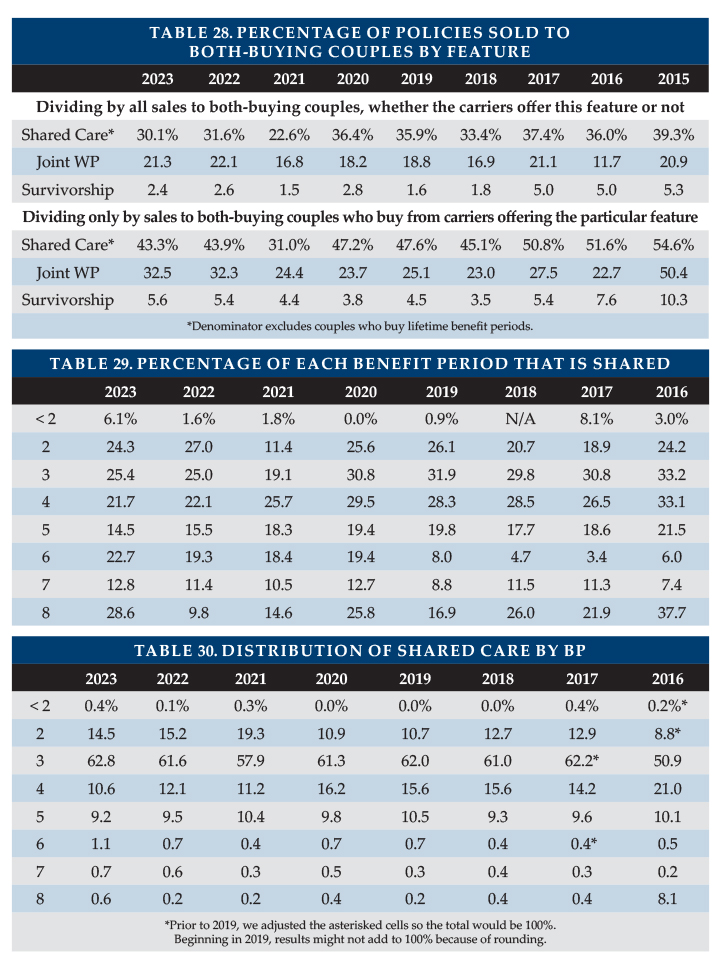
Table 21 shows lower Joint Waiver of Premium and Survivorship sales to couples in the WS market than in the NWS market. Some products automatically provide Joint Waiver of Premium if a couple buys identical coverage or if a couple buys Shared Care. Employers sometimes are disinclined to add an optional couples’ feature because they are already contributing more money to cover both a married employee and that employee’s spouse than the cost for a single employee the same age.
CLOSING We thank insurance company staff for submitting the data and responding to questions promptly. We also thank Sophia Fosdick and Quentin Clemens of Milliman for managing the data expertly.
We reviewed data for reasonableness. Nonetheless, we cannot assure that all data is accurate. If you have suggestions for improving this survey, please contact one of the authors.
Claims are the lifeblood of any insurance business. If claims are not paid accurately, promptly, and smoothly, no insurance job is justified because all insurance jobs are created fundamentally to pay clients’ claims.
In the long term care insurance (LTCI) industry, there are high-level indicators and detailed experiences that claims are paid well, but there is always room for improvement. As an industry, it is important to optimize results for the consumer and to publicize our success. Criticism, whether valid or not, lives forever on the internet. And people are generally more determined to share dissatisfaction than to describe outstanding service.
Beyond being our mission, favorable claims results are critical to the growth of the LTCI industry (including stand-alone LTCI and all types of combination products, collectively “LTCI” herein). A strong reputation for paying claims encourages producers to recommend that clients consider LTCI, encourages clients to buy and adds meaning to the lives of insurance producers (“producers” herein) and home office staff.
Producers can help by educating clients regarding claims provisions, so clients will know what to expect and also what not to expect. Such education should be refreshed upon periodic reviews. Producers can also help by finding optimal coverage for the client, which can require, among other things, detailed understanding of LTCI policy provisions.
Over time, producers can help clients recognize when a claim might be imminent and can help clients prepare for a claim and deal with their insurer effectively at claims time.
Insurers have a significant challenge. Their responsibility to pay claims promptly and smoothly must be balanced with accuracy. Overpayment of claims can lead to price increases on inforce policies and can encourage individual and coordinated fraud.
Most people recognize that existing processes can be improved. That is evident because even insurers with closed blocks of business have invested a lot of money to improve their claims practices.
In this series of articles we intend to look at many aspects of the claims process, hoping to help the industry improve and market stellar service. We’ve teamed together because we share passion for this topic and because it is daunting and benefits from multiple perspectives. We can do a better job if producers, home office staff and perhaps other readers help. At any time, readers are invited to send questions, comments, examples of favorable or unfavorable claims processing, and suggestions to either or both authors:
Here is one of Claude’s favorite claims experiences: I was about to go on a webinar when I got a phone call from a former associate who had spoken with three sisters whose mother was on claim. Naturally, claim payments were going to the claimant’s husband. But, unbeknownst to the insurer, he had repeatedly refused to pay for his wife’s care, telling his daughters that it was his money to spend as he’d like. As I had only a few moments before the webinar, I quickly left a message for a claims person at the insurer. During the one-hour webinar I saw a flurry of notices in the corner of my screen indicating communication. After the webinar I saw that the bursts of email identified the client; secured information demonstrating that claim payments should go to the daughters; and informed them that the benefit payment had been switched to them. Within an hour, the problem had been fixed!
Certainly, there are a lot of claimants/families who have been frustrated seeking LTCI claims; we’ll address at least some of those issues in this series. However, as we noted earlier, there are some high-level indicators that the industry is doing a good job.
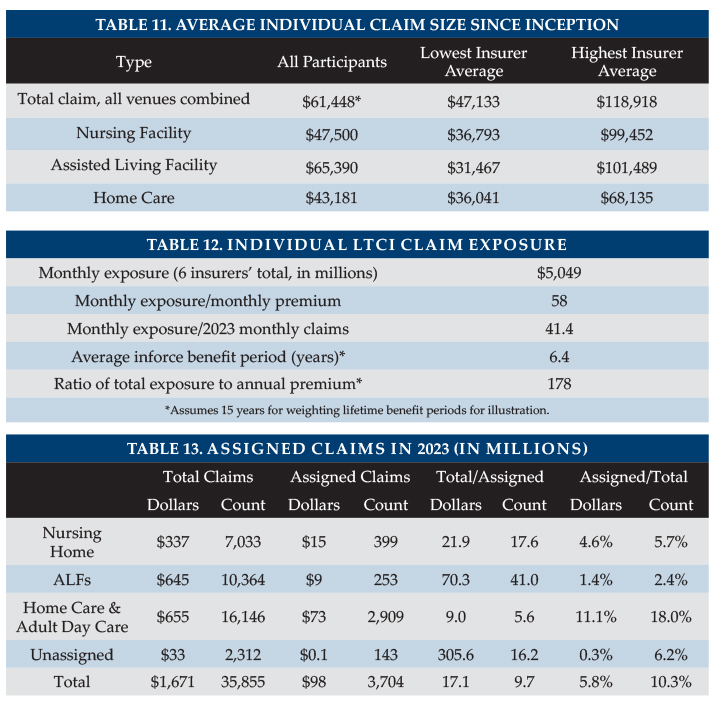
The industry has paid about $225 billion in claims, projecting from the $196 billion as of year-end 2022 reported in the 2024 Milliman Long-Term Care Insurance Survey published in Broker World magazine in July/August, 2024.
The NAIC passed Independent Review (IR) of LTCI claims to help clients get satisfaction if they think their claim was improperly denied because they were deemed not to be “chronically ill”. (For text, see p. 62+ of https://content.naic.org/sites/default/files/inline-files/committees_b_senior_issues_exposure_ltc_model_act_641.docx). Most LTCI insurers extend IR beyond statutory requirements (e.g., to policies issued prior to the effective date of IR). Nonetheless, only a very small percentage of claims go to IR. Steve LaPierre is president of LTCI Independent Eligibility Review Specialists, LLC (LTCIIERS), the largest IR organization. He reports that they upheld the insurer’s decision 98 percent of the time in 2022. It speaks well of the industry that they extend IR beyond legal requirements, that few claims go to IR and that 98 percent of those going to IR are resolved in favor of the insurer.
A 2010 study of LTCI claims payment accuracy for the Department of Health and Human Services1 found that insurers paid 3.3 percent more in claims than the auditors felt was justified under the terms of the contracts. Naturally some claims were erroneously declined, but the auditors found that the questionable claims which were paid* more than offset the claims that the auditors felt were erroneously declined. (*The auditors didn’t say those claims should not have been paid, just that there was not adequate justification in the files.) The study included seven insurers which were responsible for 70 percent of the claims at that time (Bankers Life & Casualty, Genworth Financial, John Hancock, Long Term Care Partners, Medamerica, Metropolitan Life, and Prudential.) Other insurers might have had different results.
It is ironic that we hear so much about the huge rate increases on older LTCI policies (generally those issued before 2010 and worst for those issued before 2000) but we don’t hear the flip side: State regulators would not be approving those rate increases if they were not convinced that the insurers are paying a lot more claims than they expected and will continue to do so.
Our future articles will cover topics such as:
The insurers’ perspective: Challenges they face, actions they’ve taken and areas of potential improvement.
Ways producers can help clients reduce claims, prepare for claims, recognize that claims are imminent and get claims satisfaction.
Key provisions that producers should note. (The importance of such subtleties encourages some producers to outsource LTCI sales. There are many ways producers can have very positive long term care planning conversations with clients, identifying a possible interest in LTCI before introducing their client to a specialist.)
The 2024 Milliman Long Term Care Insurance Survey is the 26th consecutive annual review of stand-alone long term care insurance (LTCI) published by Broker World magazine. It analyzes the marketplace, reports sales distributions, and describes available products. More discussion of worksite sales, including a comparison of worksite sales distributions vs. non-worksite sales distributions will be in Broker World magazine’s September/October issue.
Unless otherwise indicated, references are solely to U.S. stand-alone LTCI sales, excluding exercised future purchase options (FPOs) or other changes to existing coverage. “Stand-alone” refers to LTCI policies that do not include death benefits (other than returning premiums upon death or waiving a surviving spouse’s premiums) or annuity or disability income benefits. Where referenced, “combo” or “combination” products provide LTCI combined with life insurance or annuity coverage. “Linked benefit” policies are combo policies which can allow more than the death benefit or annuity account value to be used for long-term care (LTC).
All references to sales in terms of “premium” refer to “annualized” premium (1 x annual; 2 x semi-annual; 4 x quarterly; 12 x monthly), even if only one monthly premium was received before year-end. “WCF” refers to the “Washington Cares Fund,” explained in the Market Perspective section.
Highlights from this year’s survey As discussed in our survey of 2021 sales, the WCF stimulated tremendous market demand in the state of Washington, causing sales distributions to vary greatly from history (as one example, more sales to males than to females). In 2022, some participants’ sales distributions continued to be influenced by a backlog of 2021 applications. The 2023 sales distributions in this year’s survey should have no such influence.
Participants Seven insurers (Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian Life, New York Life, Northwestern, and Thrivent) participated, providing broadly to stand-alone sales distributions reported herein. Total 2023 sales data includes one additional contributor and 2023 inforce data includes two additional contributors.
Our worksite sales reflect the total industry, but our worksite sales distributions do not reflect low-price worksite programs; hence, our worksite sales distributions are not characteristic of the entire worksite market.
The following ten insurers contributed to our combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual (Northwestern), OneAmerica, Securian, Trustmark and United of Omaha.
Sales Summary
As seen in Table 1, contributors reported total stand-alone LTCI annualized new premium sales of $121 million in 2023 (including exercised FPOs except FPOs for insurers no longer selling LTCI and counting 10 percent of single premium), which is 2.5 percent less than the contributors’ reported sales of $124 million in 2022. The 2.5 percent drop reflects a 5.9 percent decrease for premium on new LTCI policies, partly offset by a 6 percent increase in FPOs and single premium.
The 2023 sales to 24,734 new insureds is 9 percent lower than 2022 sales to 27,181 new insureds, resulting in an 3.4 percent increase in average premium per new insured (excluding FPOs).
The percentage of 2023 sales that occurred in the worksite were the lowest ever in our sales survey. We observe that life insurance policies with LTCI or chronic illness riders are more commonly sold in this market.
Including FPO elections, Northwestern accounted for 48 percent of annualized new premium. Mutual of Omaha continued to lead in annualized premium from new policies and accounted for 30 percent of new insureds in 2023.
Although our sales survey covers essentially the entire stand-alone LTCI market, the ten insurers contributing combo sales are a smaller percentage of the combo market. LIMRA provided broader information about the combined life/LTCI market to supplement the data reported by contributors in our survey.
Reflecting nine entities’ data, the number of inforce insureds dropped 2.8 percent while annualized premium increased 0.2 percent. Inforce premium rises due to sales, price increases, and benefit increases (including FPOs), and falls from lapses, reductions in coverage, deaths, and shifts to paid-up status. The number of people with stand-alone coverage increased through 2014, but, as shown in Table 2, has decreased annually since then except for the 2021 aberration. However, inforce premium has continued to increase each year due to inforce price increases and higher prices for new policies.
Collectively, eight participants paid 9.3 percent more in claims in 2023 than in 2022. Overall, the stand-alone LTCI industry incurred $15.0 billion in claims in 2022 based on companies’ statutory annual filings, a 10.6 percent increase over 2021, which raises the running total of incurred claims since 1991 to $196.0 billion (2022 claims of $15.0 billion plus total of $180.9 billion from our prior year’s article).
About the Survey This article is arranged in the following sections:
Highlights provides a high-level view of results.
Market Perspective provides insights into the LTCI market.
Claims presents industry-level claims data.
Sales Statistical Analysis presents industry-level sales distributions reflecting data from 8 insurers.
Partnership Programs discusses the impact of the state partnerships for LTCI.
Underwriting Data discusses underwriting decisions, turn-around times and tools.
Product Exhibit shows, for 6 insurers: financial ratings, LTCI sales and inforce policies, and product details.
Product Details, a row-by-row definition of the product exhibit entries, with some commentary.
Premium Exhibit shows lifetime annual premiums for each insurer’s most common underwriting class, for issue ages 40, 50, 60, and 70 for single females, single males, and female/male couples (assuming both buy at the same age), based on $100 per day (or closest equivalent weekly or monthly) benefit, 90-day facility and most common home care elimination period, three-year and five-year benefit periods or $100,000 and $200,000 maximum lifetime buckets, with and without Shared Care and with flat benefits or automatic three or five percent annual compound benefit increases for life. Worksite premiums do not reflect any worksite-specific discount, though some carriers offer this.
Premium Adjustments (from our Premium Exhibit prices) by underwriting class for each participant.
Distribution by underwriting class for each participant. Depending upon the product shown for an insurer in the Product Exhibit, we sometimes adjust that insurer’s underwriting distribution to provide readers a better expectation of likely results if they submit an application in the coming year and to line up with the prices we display. For example, if the Product Exhibit shows only a new product which has only one underwriting class (hence one price), but the insurer’s data partly or solely reflect an older product with three underwriting classifications, we might choose to show “100 percent” in their best (only) underwriting class.
State-by-state results show the percentage of sales by state, average premium by state and percentage of policies qualifying for Partnership by state.
MARKET PERSPECTIVE (more detail in subsequent parts of the article) Washington State’s “Washington Cares Fund” (WCF) stimulated tremendous demand for private LTCI from individuals and businesses in Washington in 2021. WCF imposes a 0.58 percent payroll tax to fund a $36,500 lifetime benefit to pay for care (intended to inflate according to the Washington consumer price index) as defined in the Revised Code of Washington 50B.04. People who purchased private stand-alone or combination LTCI by November 1, 2021 could file to be exempt from the tax. Because the WCF does not require policies to be kept in force to maintain an exemption, we collected data from contributors to study cumulative lapse rates through January 2024 (varying slightly among insurers) from 2021 sales. For the purposes of summarizing data, we segmented the lapse rate data into two groups depending on the level of lapse rates outside of Washington over the more than two-year period as follows:
“Normally-low” lapses, where lapse rates outside of Washington were roughly eight percent.
“Normally-high” lapses, where lapse rates outside of Washington were roughly 42 percent.
Table 3 shows results varied between blocks with normally-low lapses and blocks with normally-high lapses (such as some worksite programs). Blocks with normally-low lapses experienced a higher lapse rate for Washington sales than corresponding sales outside Washington, 2.37 times as much for stand-alone policies and 1.78 times as much for combo policies. On the other hand, blocks with normally-high lapse rates showed lapse rates were 39 percent lower for Washington sales than corresponding sales outside Washington. Early policy duration lapse rates that are higher (lower) than anticipated may depress (increase) unit profitability, as renewal premium flow is reduced. Underwriting and issue expenses are harder (easier) to amortize.
Table 4 shows the concentration of sales in Washington (for premiums and lives) from 2015 to 2023. In 2023, Washington sales continued to account for a higher percentage of new business (three percent of premium and 4.2 percent of lives) than in 2015-2019 (2.3 percent of premium and 2.4 percent of lives). As Washington’s market share of lives increased more than its market share of premiums, Washington’s average premium has lowered compared to other jurisdictions. Six of the seven insurers that contributed state distributions showed significantly larger Washington market share (in terms of new policies sold) in 2023 than in 2019.
Based on conversations with some brokers (special thanks for Carolyn Olson for her insights), we believe many people bought new larger policies in 2023 to replace small policies originally purchased in 2021. We will continue to monitor Washington’s market share in future years.
Table 5 shows the sales market share (for premiums and lives) from 2015 to 2023 in two neighboring states to Washington—Idaho and Oregon—to analyze the sales impact of the WCF in these states. Note in 2022, the WCF was amended to allow out-of-state residents who work in Washington to file for an exemption.
Our Idaho data continues to show increased market share in 2023 compared to 2020 and prior, whereas Oregon shows little difference across the years. However, as noted above, our jurisdiction distributions do not reflect the worksite-focused insurers; inclusion of worksite data might have shown more impact in Idaho and Oregon.
Table 6 shows the sales market share (for premiums and lives) from 2015 to 2023 in California to analyze whether there was any impact on sales due to the feasibility studies examining a potential new statewide LTCI program1,2. The most recent study was completed in 2023, in response to California AB5673 signed in October 2019, which called for a task force (TF) to “examine the components necessary to design and implement a statewide long term care insurance program.” The TF’s first meeting was in March 2021 and as it proceeded, more and more publicity ensued. As one example of the increased publicity, in August 2023, California Insurance Commissioner Ricardo Lara issued a warning letter4 regarding complaints related to “misleading marketing and communications by some long term care insurers and agents in connection with the work of the California Long Term Care Insurance Task Force.”
If the TF work stimulated sales, we might expect younger people to buy private LTCI and California’s market share by number of lives to increase more than its market share of annualized premium (similar to the pattern observed for Washington sales in 2021). Table 6 does appear to exhibit some of this pattern in recent years. In 2023 California’s market share by number of lives is the second highest and its market share by premium is the second lowest since 2015 (ignoring the 2021 aberration influenced by Washington sales).
To help provide perspective on the stand-alone market, we continued our recent history of reviewing life insurance sales with LTC-related provisions. These include:
“Chronic Illness Acceleration” represents features which qualify under §101(g). They are prohibited to be marketed as LTCI per NAIC regulation, hence do not require brokers to be LTCI-certified. They allow a portion of the death benefit (depending on the product, perhaps as much as 100 percent) to be used for LTC-related expenses and generally use a cash-indemnity design.
“LTCI Acceleration” features under §7702(B) can be marketed as LTCI and require brokers to be LTCI-certified. They allow a portion of the death benefit (usually one to four percent per month, generally up to 100 percent of the death benefit) to be used for LTC.
“Linked-Benefit” features allow more than the death benefit to be used for LTC, in one (or both) of two ways. First, they might include automatic annual increases to maximum benefits (such as simple or compound increases), where the additional benefits may (or may not) reduce the death benefit. Second, they may continue LTC benefits even after the death benefit has been used up. Nearly all linked-benefit purchasers in 2022 (98.2 percent according to LIMRA) chose either benefit increases or extension of benefits or both.
Although we cover essentially the entire stand-alone LTCI market, the ten insurers contributing combo sales are a much smaller percentage of the market, hence may not be characteristic of the full market. One insurer reported a much lower average size in 2023, after having reported first-year dump-ins as new annualized premium in 2022. If we remove that outlier, the increase in annualized premium was 38 percent and the increase in policies sold was 26 percent, reflecting a 9.2 percent increase in average premium to $2,965. The increase in average new premium may reflect more 10-year-pay policies, an older average issue age, etc. Prices in the market have been dropping, resulting in a lower cost for whatever monthly maximum LTC benefit is desired. It is particularly interesting that the average premium rose despite the lower unit prices. Our single premium combo participants experienced a 5.4 percent increase in new annualized premiums, an 3.5 percent increase in the number of policies sold, and a 1.8 percent increase in average premium per policy. We do not get statistical breakdown of combo sales.
LIMRA kindly shared its 2022 combination product sales findings. Tables 7 and 8 summarize the stand-alone LTCI data from our survey alongside the LIMRA combination product data. Table 8 shows that 89.5 percent of the recurring premium policies (and more than 90 percent of the associated premium) with a LTCI-related feature were limited to acceleration of the death benefit. Of these, the vast majority were Chronic Illness riders because they can be added at no cost and without limiting distribution to LTCI-certified brokers.
Of the policies that can be marketed as LTCI, 68 percent of the recurring premium policies are on policy forms that offer only LTCI Acceleration features, whereas 96 percent of the single premium policy forms also offer extended LTCI benefits after the death benefit has been used up as LTCI.
Linked-Benefit (referred to as “LTCI Extension” by LIMRA) sales together with Stand-alone LTCI sales account for 12.4 percent of policies (including single premium policies).
Our 2022 data differs from LIMRA because we had fewer insurers and more worksite sales with chronic illness features. Excluding worksite, we have 55 to 60 percent of LIMRA’s Linked-Benefit sales and a similar average size, adjusting for the carrier that reported dump-in premium as on-going. Similarly, we have about 40 percent of recurring premium policies with LTCI Acceleration and a similar average size, but have a very small portion of LTCI Acceleration single premium policies.
Excluding our worksite policies, we have 20 percent of LIMRA’s Chronic Illness cases, but only half as much premium. Adding our worksite policies, we have 45 percent of Chronic Illness cases but only 13 percent of premium because worksite cases have much lower premium.
Linked benefit and other combination products are attractive to consumers because if the insured never has an LTC-related claim, their beneficiary will receive a death benefit. They also are more likely than stand-alone LTCI to have indemnity benefits and guaranteed premiums.
Such policies generally cost more than stand-alone LTCI if there is comparable LTCI coverage at older ages (such as age 85). However, the price difference seems to be shrinking because higher interest rates and competition appear to be driving linked-benefit prices lower while stand-alone LTCI new business prices have generally increased in recent years, especially for one-of-a-couple sales. Because of their benefit increase features, stand-alone and linked-benefit products often provide more LTC protection at older attained ages than policies which provide LTCI only through an accelerated death benefit.
In 2023, 59.3 percent of stand-alone LTCi applications went inforce, the second straight increase since an all-time low of 54.1 percent (excluding Washington applications in 2021. Nonetheless, some may still view the placement rate as problematic. Prior to 2009, two-thirds of applications were placed despite higher average issue ages (however, in that era, there were more worksite cases with limited underwriting).
Higher placement ratios are critical to encourage financial advisors to mention LTCI to clients. The following opportunities can improve placement rates.
E-applications, which can speed submission and reduce processing time.
Uploading medical records via human application program interface (API).
Health pre-qualification by distributors, which can be aided by drill-down questions in on-line underwriting guides.
Requiring cash with the application.
Improved messaging regarding the value of LTCI and of buying now (rather than in the future).
Beyond Washinton and California, other states have taken action recently regarding possible state-run LTCI programs. Examples include:
Minnesota received a contractor’s report regarding options to increase access to long term care financing, services, and support.
New York SB 462 and Pennsylvania HB 844 would establish state insurance programs.
Kentucky HR 100, Massachusetts HB 652, and Vermont H.444 would establish bodies to study feasibility of a state insurance program. Connecticut SB245 would study LTC needs, not specifically LTCI.
Future state LTCI programs will likely differ from WCF in several respects. For example, based on draft laws and task force discussions in other states, they:
May not leave the window open for people to opt out by buying LTCI after the legislation has been signed.
May require that private LTCI policies remain in force to maintain exemption.
May narrow the range of private LTCI policies that qualify for exemption.
The FPO (future purchase option, a guaranteed, or a non-guaranteed board-approved, option, under specified conditions, to purchase additional coverage without demonstrating good health) election rate rose to 86.3 percent, which is in line with what the same insurers reported in the past.
Considering such FPOs and other increased coverage provisions, we project a maximum benefit at age 80 of $334/day for an average 57-year-old purchaser in 2023, which is equivalent to an average 2.9 percent compounded benefit increase between 2023 and 2046. Inflation appears to be more of a concern now. As discussed later, purchasers may be disappointed if the purchasing power of their LTCI policies deteriorates over time.
Current premiums are much more stable than past premiums, partly because today’s premiums reflect much more conservative assumptions based on far more credible data. The Policy Exhibit shows, for each insurer, how long ago the most recent policy was issued that has had a price increase and how long ago the currently-issued product was priced. No participant has raised prices for policies issued in 2017 or later. Additionally, it has been three years since any participant released new prices for new sales. Financial advisors may not be familiar with the greatly improved stability of LTCI premiums, hence may be reluctant to encourage clients to consider LTCI because the advisors fear steep price increases.
Some insurers of older inforce polices are also exploring strategies around rate stability. As one example, New York Life made old inforce blocks non-cancelable (guaranteed to have no future rate increases) in states which approved their full most recent (second) rate increase on those policies, even if the increase was required to be phased in over several years. This premium rate guarantee even applies to the oldest policyholders (ages 74 and older) who were exempted from the rate increase.
All insurers in our Product Exhibit offer coverage in all U.S. jurisdictions, except two of them do not offer policies in New York. This year, we asked insurers how many declines are successfully appealed. Three insurers responded, with percentages ranging from 2.7 to four percent. We asked what percentage of “non-frivolous” underwriting appeals are reversed, a question which insurers likely interpreted differently. One insurer’s data indicated 37 percent while another’s indicated 82 percent.
CLAIMS Independent Third-Party Review (IR) is intended to help assure that LTCI claims are paid appropriately. Since 2009 (in some jurisdictions), if an insurer concludes that a claimant is not chronically ill as defined in the LTCI policy, the insurer must inform the claimant of his/her right to appeal to IR, which is binding on insurers.
In many states, IR is not effective, either because the law was not adopted or because regulators have not set up the required panel of independent reviewer organizations (IROs). Nonetheless, a claimant could ask an insurer to agree to IR.
The Product Exhibit shows that most participants extend IR beyond statutory requirements (e.g., to policies issued prior to the effective date of IR). Some insurers hire IROs to provide another set of eyes as part of the insurer’s internal appeal process.
A very small percentage of claims go to IR. Some insurers say they have never had a request for IR.
We are not aware of regulators who track IR results, but Steve LaPierre, President of LTCI Independent Eligibility Review Specialists, LLC (LTCIIERS), the largest IR organization, reports that they upheld the insurer’s decision 98 percent of the time in 2022.
For comparison, a National Nurses United study of CA acute health claims1 indicates that IR upheld half of their denials. Acute health insurance and LTCI claims are denied for different reasons which likely explains much of the difference in the rate at which the insurers’ decisions are overturned.
The LTCI industry’s IR experience suggests that insurers, overall, are paying claims appropriately.
Eight participants reported 2023 claims. As some companies are not able to provide complete detailed data, some statistics reported below are more robust than others.
The eight entities’ combined individual and multi-life and group claim payments were 9.3 percent higher than in 2022, based upon 1.9 percent more claimants, resulting in a 7.2 percent increase in the average individual and multi-life claim payment. The average group claim payment saw a much larger 29 percent increase but reflects more volatility from a smaller number of claimants.
The LTCI industry has paid out benefits to policyholders far greater than indicated in the following statistics, because most claims are paid by insurers that do not currently sell LTCI.
Our claims represent about 10 percent of claims paid by the industry. LTCI claims paid by insurers no longer selling LTCI may differ significantly from the following statistics as their claimants are more likely to have facility-only coverage, be older, and/or have other different policy or demographic characteristics.
Table 9 shows the total dollar and number of reported individual and multi-life (not group) LTCI claims. Table 10 shows the percentage paid by venue. In both tables, “since inception” means since the insurer first started selling LTCI or as far back as they can report these results (for example, they may have changed claims administration systems and not be able to go all the way back to when they first processed claims).
Table 10 shows that home care and adult day care (collectively “HC” in Table 10) account for the highest percentage of 2023 claims (38.7 percent) but the second-most percentage of 2023 claim dollars (30.3 percent). Assisted Living Facilities (ALFs) account for the second-most percentage of 2023 claims (35.3 percent) but the highest percentage of claims dollars (40.0 percent). Despite the shift away from nursing homes to ALFs, nursing homes still account for the largest percentage of inception-to-date claims numbers (47.5 percent) and claims dollars (46.0 percent).
Trends can be obscured because different insurers may report claims data over the years and insurers refine how they report data. For example, we learned in 2021 that one insurer previously assigned all of a claimant’s benefits based on the venue in the claimant’s first month of claim, which implies the shift from NH to ALF since 2020 is greater than the table indicates.
In the distribution based on number of claims, a person who received care in more than one venue is counted once for each venue, but not double-counted in the total line. The average claimant is in 1.5 types of venues during the course of the claim; this does not recognize multiple providers within a single type of revenue (e.g., two nursing homes).
Six carriers reported the number of open individual claims at year-end. Open claims at year-end 2023 averaged 78 percent of the number of claimants served at any point during 2023, an increase from 70 percent the past few years.
Table 11 shows average size individual claims since inception: that is, including older claims and reflecting all years of payment. One participant refined its reporting this year, causing comparisons to prior years to not be meaningful.
Because some claimants submit claims from more than one type of venue, the average total claim might be expected to exceed the average claim paid for any particular venue. Individual ALF claims stand out as high each year, probably because: a) ALF claims appear to have a longer duration compared with other venues. b) Nursing home costs are most likely to exceed the policy daily/monthly maximum, hence nursing home claims are most likely to understate actual cost of care. c) People who maximize the use of their maximum monthly benefits can generally spend as much in an ALF as in a nursing home. d) Although some surveys report that on average ALFs cost about half as much as nursing homes, ALFs may have an extra charge for a memory unit or for levels of assistance that align more closely with nursing home care.
Several insurers extend ALF coverage to policies which originally did not include ALF coverage, providing policyholders with significant flexibility at the time of claim but contributing to the insurers’ need for rate increases.
The following factors contribute to a large range of average claim by insurer (see Table 11):
Different markets (by affluence; worksite vs. individual; geography; etc.)
Demographic differences (gender; issue age; age of their block of business)
Distribution by benefit period, benefit increase feature, shared care, and elimination period. For example, one carrier has a higher average home care claim than its average facility claim, because people who added the home care rider were more likely to add compound “inflation” also.
Distribution by facility-only policies vs. 50 percent home care vs. 100 percent home care vs. home care only.
Differences in the ways insurers report claims.
The following factors cause our average claim sizes to be understated:
Approximately 16 percent of inception-to-date individual claims are still open and our data does not include reserve estimates for future payments on open claims.
People who recover, then go on claim again, are counted as multiple insureds, rather than adding their various claims together.
Besides being understated, average claims data does not reflect the value of LTCI benefits from some purchasers’ perspectives, because the many small claims drive down the average claim. LTCI provides significant financial yield for most people who need care one year or longer. A primary purpose of insurance is to protect against adverse results, so the amount of protection, as well as average claim, is important.
Six insurers provided current individual monthly LTCI claim exposure (note: the data reflects only initial monthly maximum for one insurer). As shown in Table 12, this figure is 28 times their corresponding monthly LTCI premium income and 41.4 times their 2023 LTCI monthly paid claims. Seven insurers contributed inforce distribution by benefit period. Treating endless (lifetime benefit periods) as a 15-year benefit period, their average inforce benefit period has reduced to 6.4 years, ignoring Shared Care. Increasing the assigned value of the endless benefit period by one year raises the average inforce benefit period approximately 0.23 years. With annual exposure 28 times annual premium and an average benefit period of 6.4 years, we estimate total exposure is 178 times annual premium.
The current average individual maximum monthly maximum benefit for claimants seems to be in the $4,900 to $8,500 range. Nursing home (NH) claims are more likely to use the policy’s maximum daily/monthly benefit than ALF claims because ALF daily/monthly costs are generally lower and because policies sometimes have lower maximums for ALFs. ALF claims correspondingly are more likely to use the policy maximum than are adult day care and home care claims.
A person might think LTC providers can fully answer the question “how much do insurers pay for LTC?” However, providers likely know only how much they receive from insurers (assigned payments), not amounts clients pay that is subsequently reimbursed from insurers. In this year’s survey, we decided to study assignments (Table 13). Five insurers contributed data.
Based on 35,855 claims, the reported data indicated 5.8 percent of claims dollars and 10.3 percent of the count of claims were assigned; in other words, total claim dollars are roughly 17 times what is assigned to providers and the total number of claims is 10 times the number that are assigned. We asked two insurers with large closed blocks (each larger than the data in our table) for their experience as additional data points for comparison. One insurer estimated similar percentages: roughly six percent of facility claim dollars and roughly 10 percent to 15 percent of home care claim dollars were assigned. The other insurer estimated that roughly 13 percent of their claim dollars were assigned.
Home care claims are roughly 4.5 times as likely to be assigned as facility claims, and, for each venue, small claims are more likely to be assigned than large claims.
It may be disadvantageous for providers when nursing home claims are assigned if the LTCI policy does not cover the full provider rate, as the provider would have to bill the family as well. Insurers may not prefer facility claims to be assigned if the facilities want to be paid in advance; in addition to the loss of potential investment income, insurers have difficulty recovering overpayments if a claimant does not stay in the facility for the full month. In contrast, home care claims are billed in arrears and policy benefit limits are more likely to exceed home care charges than nursing home charges.
SALES STATISTICAL ANALYSIS Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian, New York Life, Northwestern and Thrivent contributed significant background stand-alone LTCI sales data, but some were unable to contribute some data. LifeSecure provided only total stand-alone sales, not distributions.
Sales characteristics vary significantly among insurers based on market differences (individual vs. worksite, affluence, gender distribution, etc.). Year-to-year variations in policy feature distributions may reflect industry trends but may also reflect changes in participants, participant practices and designs, participant or worksite market shares, etc. The 2021 sales also exhibit major variance from historical results due to Washington sales. Statistical differences between the worksite and non-worksite sales will be reported in the September/October issue of Broker World.
Market Share We include purchased increases on existing policies as new premium because new coverage is being issued. Table 14 shows 2023 new premium, both including and excluding FPOs.
The stand-alone market continues to consolidate, as well as shrink. Northwestern accounted for 48 percent of annualized new premium, while Mutual of Omaha maintained its lead in annualized premium from new policies (by $100k) while continuing to sell the most policies (29 percent; see Policy Exhibit). The top 3 insurers had 84 percent market share, compared to 81 percent in 2022 and 74 percent in 2021. Excluding FPOs, the concentration is lower, 80 percent in 2023. The premium in table 14 includes 100 percent of recurring premiums plus 10 percent of single premiums.
Worksite Market Share and Average Premium The percentage of 2023 sales that occurred in the worksite was the lowest ever, with four insurers reporting 2023 worksite sales. The worksite market has gravitated toward life insurance policies with an accelerated death benefit, as will be covered in the September/October article.
Worksite sales normally consist of three different markets as outlined below, the first two of which produce a higher percentage of new insureds than of new premiums.
Voluntary group coverage generally is less robust than individual coverage.
Core/Buy-Up programs have particularly young age distributions and modest coverage because a lot of people do not buy-up and are less likely to insure spouses.
Executive carve-out programs generally provide the most robust coverage. One-or two-couple executive carve-out sales may not qualify for a multi-life discount with some insurers, hence may not be labeled as worksite sales in submissions to our survey.
The amount of worksite sales reported, the FPO activity, the degree to which insurers report worksite distributions, and the distribution of worksite sales among the above-described sub-markets significantly impact sales characteristics. Our participants’ (insurers which provided sales distributions) average annual premium on new worksite policies was $2,271, but contributors that provided sales, but not distributions, had an average premium of $1,476. That average premium discrepancy makes clear that our sales distributions do not reflect the insurers focusing in the group voluntary and core/buy-up markets.,
The 5.9 percent of premium attributed to worksite sales in Table 15 includes FPOs. Limiting all premium to new policies, the worksite premium market share is 3.2 percent. More information about worksite sales will appear in Broker World magazine’s September/October issue.
Affinity Market Share Affinity groups (non-employers such as associations) produced 5.4 percent of participants’ 2023 premium and 7.2 percent of policies.
Characteristics of Policies Sold Average Annualized Premium Per Sale To determine the average annualized premium for new sales, we exclude FPOs and single premium policies, except where noted otherwise. As shown in Table 17, the average premiums in 2022 and 2023 have been higher relative to historical because of fewer small worksite policies and higher unit prices post-2020.
The influence of small worksite policies is greatly reduced now. Removing the primary insurer in that market produces an average premium per insured of $3,375, as shown in Table 17. Including this carrier produces an average premium of $3,342. Note, the difference between the average premium per buying unit and per insured is larger in the individual market because the individual market has more couples who both buy, which influences the results in Table 17 when reviewing results across the total market and individual market.
The jurisdiction with the lowest average new premium for participants in 2023 (including FPOs and counting 100 percent of single premiums) was Washington ($3,609), followed by Puerto Rico ($3,850), and Mississippi ($3,954). The jurisdiction with the highest average premium was Connecticut ($7,211), which would have been third if single premiums were excluded, followed by Wyoming ($7,167), Minnesota ($6,585), North Carolina ($5,991), Pennsylvania ($5,971) and Illinois ($5,926).
Issue Age Table 18 shows the average issue age remained 57.1. Note: one survey participant has a minimum issue age of 40, one will not issue below 30, and one will not issue below 25.
Benefit Period Table 19 shows that the average benefit period remained similar to last year, with the largest changes occurring for the 4-year and 6-year policies.
Monthly Benefit Monthly determination continued to be roughly 78 percent of new policies (Table 20). With monthly determination, low-expense days preserve more coverage to use for high-expense days, offering more flexibility for insureds. One insurer offers only daily determination; one insurer offers a choice; and the other insurers automatically have monthly (or weekly) determination.
Sales in 2023 set a record average maximum monthly benefit ($5,168), as shown in Table 21. Sales with an initial monthly maximum of $9,000 or more ranged from a low of three percent of sales for one insurer to a high of 13.3 percent for another.
Benefit Increase Features Table 22 generally shows reduced inclusion of pre-paid benefit increase features (i.e., total of rows in Table 22 excluding sales for no benefit increases and FPOs) in 2023 stand-alone LTCI policies.
“Indexed Level Premium” policies are priced to have a level premium, but the benefit increase is tied to an index such as the consumer price index (CPI).
A person’s amount of LTCI coverage in their elder years is critical. Therefore, each year, we estimate the amount of coverage an average buyer would have at age 80. We project the age 80 maximum daily benefit by increasing that year’s average initial maximum daily benefit (MDB) from the average issue age to age 80, according to that year’s distribution of benefit increase features, using current future purchase option (FPO) election rates and a five percent per year offer for fixed FPOs. Table 23 shows the projected maximum benefit in 2046 (at age 80) for our 2023 average 57-year-old purchaser ($334/day; equivalent to 2.9 percent compounding) and corresponding results for prior years.
To compare the eventual purchasing power of each year’s average purchase, we used the same methodology to estimate the maximum daily benefit in 2046, also shown in Table 23. While an average 2023 buyer would have $334 of MDB in 2046, an average 2022 buyer would have $319 of MDB and an average 2021 buyer $259 of MDB, but an average 2020 buyer would have $345 of MDB.
With greater potential concern about inflation given the current economic environment, consideration of benefit increases likewise may grow more important. People are likely to be disappointed if cost of care grows faster than the protection built into their policy.
FPOs (Table 24) can play an important role in maintaining insureds’ purchasing power. In 2023, 86.3 percent of FPOs were elected, generally in-line with these contributing insurers’ prior experience. The high election rate is particularly noteworthy as the cost increases each year due to larger coverage increases each year, increasing unit prices due to age, and possibly rate increases.
Negative-election FPOs activate automatically unless the client rejects them. Positive-election FPOs activate only if the client initiates a timely request. The high election rate reflects the effectiveness of annual (as opposed to triennial) negative-election provisions (particularly those which can be lost prospectively if not currently exercised) and may reflect the importance of LTCI to policyholders, especially in an inflationary environment.
One participant had an election rate over 90 percent, but two insurers had election rates of 27 to 29 percent. FPOs can also be important to insurers as well. One insurer got 58 percent of their new premium from FPO elections.
Elimination Period Table 25 summarizes the distribution of sales by facility elimination period (EP), which shows some increasing trend for EPs of 200+ days. Two insurers saw more than five percent of their buyers chose EPs longer than 200 days.
Table 26 shows the percentage of new policies with zero-day home care elimination period (but a longer facility elimination period). The purchase rate of an additional-cost zero-day home care EP option is sensitive to the price. The higher percentages prior to 2021 reflect an insurer which stopped selling LTCI.
Table 26 also shows the percentage of new policies with a calendar-day EP. Calendar-day EP provisions count a day toward the EP if you need care, even if you do not get commercial care. Service-day EPs count only days on which commercial care is received. However, most calendar-day EP provisions require an up-front paid-service day to start counting.
Sales to Couples and Gender Distribution Table 27 summarizes the distribution of sales by gender and partner status. The sales show a smaller percentage (71.7 percent in 2023 vs. 78.3 percent in 2022) of healthy spouses bought policies when their partner was declined. Otherwise, the 2023 sales distributions were similar to 2022.
Shared Care and Other Couples’ Features Table 28 summarizes sales of Shared Care and other couples’ features.
Shared Care allows one spouse/partner to use the other’s available benefits if their own coverage has been depleted or offers a third independent pool the couple can share.
Survivorship waives a survivor’s premium after the first death if specified conditions are met (such as having been inforce for 10 or more years).
Joint waiver of premium (WP) waives both insureds’ premiums if either insured qualifies for benefits.
Changes in distribution by carrier can greatly impact year-to-year comparisons (Table 28). Some insurers embed survivorship or joint waiver automatically (sometimes only for particular circumstances such as if Shared Care is purchased), while others offer it for an extra premium or do not offer the feature.
In the top half of Table 28, percentages are calculated based on the total number of policies sold to couples who both buy (for Shared Care, only those who buy a limited benefit). The percentages in the bottom half of Table 28 reflect only the sales from insurers offering that particular feature.
For insurers reporting Shared Care sales, the percentage of both-buying couples who opted for Shared Care varied from 9.9 percent to 72.1 percent. The corresponding percentage of couples with Joint WP varied from eight percent to 100 percent and for Survivorship ranged from 2.5 percent to 14.2 percent.
Tables 29 and 30 provide additional breakdowns on the characteristics of Shared Care sales. Table 29 shows the percentage of each benefit period that included Shared Care. Table 29 shows low percentages of Shared Care, partly because its denominator includes all policies, even those sold to single people or one of a couple.
Table 30 looks only at Shared Care policies and reports their distribution across benefit period, so the percentages must total 100 percent. As most policies have three-year benefit periods, most Shared Care policies had a three-year benefit period.
Shared Care is generally more concentrated in two- to four-year benefit periods than are all sales. Couples often buy shorter benefit periods because they plan to help care for each other and expect the male partner to not need care for a long time. With Shared Care, if the male dies without using all his coverage, his unused coverage is available for the surviving female. As shown in Table 27, single buyers are more likely to be female and females are more likely to opt for a longer benefit period.
In 2023, sales generally showed a downtick in the percentage of short benefit period policies that included Shared Care and saw an uptick in Shared Care among longer benefit period policies.
Existence and Type of Home Care Coverage Three participants reported sales of facility-only policies, which accounted for 0.4 percent of total sales. For many years, one insurer has been responsible for more than 80 percent of such sales. Most (96 percent) comprehensive policies included home care benefits equal to the facility benefit, while the other policies had a home care benefit at least 50 percent of the nursing home benefit. The most recent home-care-only sale in our survey was sold in 2018.
Other Characteristics Two insurers offer Partial Cash Alternative features, which allow claimants, in lieu of any other benefit that month, to use 25 to 30 percent of their coverage for whatever purpose they wish. Table 31 shows Partial Cash Alternative features were included in fewer policies due to a change in market share among participants.
Two insurers offer an additional (not an alternative as indicated above) benefit that is a cash benefit. Only 0.3 percent of polices included that feature.
Return of premium (ROP) features were included in 8.5 percent of policies. ROP returns some or all premiums (usually reduced by paid LTCI benefits) when a policyholder dies. Roughly 74 percent of ROP features were embedded automatically in the product. Embedded features are designed to raise premiums minimally, typically decreasing the ROP benefit to $0 by age 75. For the survey participants, 20 percent of ROP features would pay benefits for death after age 75.
Restoration of Benefits (ROB), which restores used benefits when the insured has not needed services for, typically at least six months, was included in 17.2 percent of policies with limited benefit periods. Roughly 90 percent of ROB features were automatically embedded.
Insurers must include shortened benefit period (SBP) coverage unless buyers specifically decline the feature. SBP coverage makes limited future LTCI benefits available to people who stop paying premiums after three or more years. Most (95.8 percent) buyers refused SBP. (Note: Contingent SBP coverage is included automatically at no cost.)
Only one insurer issued non-tax-qualified (NTQ) policies, which accounted for 0.1 percent of total industry sales.
“Captive” (dedicated to one insurer) agents produced 61.8 percent of the sales. Brokers produced the balance. At one time, “captive” agents who sold LTCI tended to specialize in LTCI. Now many are agents of mutual companies.
Limited Pay and Paid-Up Policies In 2023, two insurers in the survey sold policies that become paid-up in 10 years or less, accounting for 1.2 percent of sales.
Because today’s premiums are more stable compared to policies sold years ago, premium increases are less likely. One of the key reasons for buying 10-year-pay (avoidance of rate increases after the 10th year) is greatly reduced, while the cost of 10-year-pay has increased, making it less attractive for consumers than in the past. Nonetheless, limited-pay and single-pay policies are attractive to minimize post-retirement outflow and to accommodate §1035 exchanges.
Eight participants reported that roughly four percent of their 2023 inforce policies are paid-up, similar to 2022.
When someone applies to Medicaid for long term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (some Indiana and New York policies disregard all assets). Except for California, states with Partnership programs grant reciprocity to Partnership policies issued in other jurisdictions. Partnership programs are approved in 44 jurisdictions, all but AK, DC, HI, MA, MS, UT, and VT. However, MA has a similar program (MassHealth).
Four states (CA, CT, IN and NY) blazed the trail for Partnership programs in the early 1990s. Other states were allowed to adopt simplified and more standardized Partnership regulations by the Deficit Reduction Act of 2005 (DRA).
More than 60 percent of Partnership states allow one percent compounding to qualify for Partnership, which can help low-budget buyers qualify for Partnership and also enable worksite core programs to be Partnership-qualified. A higher percentage of policies will qualify for Partnership in the future if insurers and advisors leverage these opportunities. Currently three insurers offer one percent compounding.
Partnership programs could be more successful if:
Advisors offer small maximum monthly benefits more frequently to middle-income individuals. For example, a $1,500 initial maximum monthly benefit covers about 1.5 hours of home care per day and, with compound benefit increases, may maintain buying power. Many middle-income individuals would like LTCI to help them stay at home while not “burning out” family caregivers and could be motivated further by Partnership asset disregard. (This approach does not work in CA, CT, IN and NY because of their high Partnership minimum daily benefit requirements.)
Middle-income prospects were better educated about the importance of benefit increases to maintain LTCI purchasing power and qualify for Partnership asset disregard.
The four original Partnership states migrate to DRA rules.
More jurisdictions adopt Partnership programs. (AK, HI, MA, MS, VT, and DC do not have Partnership programs, but MA has its MassHealth program which is similar.)
Programs that privately finance direct mail educational LTCI content from public agencies were adopted more broadly.
Financial advisors were to press reluctant insurers to certify their products and offer one percent compounding.
More financial advisors were certified. Some people argue that certification requirements should be loosened. At a minimum, the renewal certification process could be improved.
Linked benefit products became Partnership-qualified.
PARTNERSHIP PROGRAM SALES Participants reported Partnership sales in 41 states, all Partnership-authorized states except CA, CT and NY. No insurer reported Partnership sales in more than 38 states and one insurer issues no Partnership policies.
Insurance brokers do not have access to Partnership policies in CA, CT and NY and from only one insurer in IN. However, consumers may be able to purchase Partnership-qualified coverage from another entity.
As shown in the Sales Distribution by Jurisdiction table of participants sales in DRA states, 46.4 percent qualified for the Partnership. Rhode Island (75.8 percent) exceeded perennialleader Minnesota (74.1 percent) for the highest percentage of Partnership-qualified sales. Maine (73.5 percent) also had more than 70 percent and North Dakota had 69.9 percent. Ten states had between 60.0 percent and 62.5 percent and another nine had more than 50 percent but less than 60 percent qualify. Fifteen states had 20 to 50 percent qualify. New Mexico (7.6 percent), Utah (12.0 percent), Indiana (13.6 percent) and West Virginia (18.7 percent) were the only DRA states in which fewer than 20 percent qualified.
UNDERWRITING DATA Case Disposition Five insurers contributed application case disposition data to the survey (Table 33). Case resolutions improved in 2023 with 59.3 percent placed and 24.9 percent declined or deferred, compared with 58.2 percent and 25.7 percent in 2022. One insurer placed 77 percent of its cases; the others placed 47 to 56 percent.
Of cases which were resolved, 27.8 percent were declined or deferred, with the percentage varying from 14.2 percent to 36.1 percent, depending on insurer. To the degree that a declined applicant got coverage elsewhere or a deferred applicant was ultimately approved, the eventual placement rate for applicants is higher than our data indicates.
Overall, 15.8 percent of cases were suspended or withdrawn during underwriting or not accepted or dropped during the free look period. That is the lowest percentage since 2019.
Factors such as age distribution, distribution system, market, underwriting requirements, and underwriting standards affect these results.
Table 34 shows the placement rate by applicant age. This data is a subset of the data in Table 33 and the “All Ages” line, as some carriers cannot provide this data by age. While the placement rate increased overall (i.e., all participants, all ages combined), the placement rate for the insurers that provided data by age decreased for ages above 40.
Low placement rates increase insurers’ cost per placed policy. More importantly, low placement rates discourage advisors from discussing LTCI with clients. In addition to not wanting to waste time and effort, advisors may fear that declined clients will be dissatisfied. In the Market Perspective section, we listed ways to improve placement rates. This is a critical issue for the industry. If readers have suggestions, they are invited to contact the authors.
Underwriting Tools Five insurers contributed data to Table 35, which divides the number of uses of each underwriting tool by the number of applications processed. For example, the number of requested medical records was 84 percent of the number of applications. Fewer than 84 percent of applications involved medical records, because some applications involved multiple medical records.
Year-to-year changes in distribution of sales among insurers significantly impact results. Lower maximum ages result in fewer face-to-face exams. Insurers might underreport the use of an underwriting tool because they may lack a good source for that statistic. For example, an insurer might not be able to split phone interviews by whether or not they include cognitive testing.
Underwriting Time Table 36 shows that for five insurers, the average processing time, from receipt of application to mailing the policy, decreased to 47 days. Rating Classification
Table 37 suggests continued overall trend to issue policies with an insurer’s “better,” lower priced underwriting classification. The percentage of decisions either declined or placed in the 3rd-Best or “less-attractive,” higher priced classifications reduced consistently. For each issue age group, Table 38 shows the percentages of policies issued in the most favorable category and Table 39 shows the decline rate. These tables do not exactly match Table 37 because some participants provide all-age data, rather than separating it by age. The percentage placed in the most favorable classification continues to generally improve within each issue age group, which may be at least partly attributable to fewer insurers offering preferred discounts compared to the past.
For each issue age group, Table 39 shows the percentages of policies declined. The decline rate dropped in 2023 for most age groups. For the past 4 years, the percentage placed in the most favorable classification has been higher for ages 75+ than for ages 70-74 and the decline rate has been lower. The age 75+ block is the smallest and most susceptible to statistical fluctuation, but the primary cause appears to be different distribution of insurers by age. For example, some insurers do not have a “preferred” health discount; the bulk of their policies are issued in their “most favorable” class.
CLOSING We thank insurance company staff for submitting the data and responding to questions promptly. We also thank Sophia Fosdick and Quentin Clemens of Milliman for managing the data expertly.
We reviewed data for reasonableness and insurers reviewed their product exhibit displays. Nonetheless, we cannot assure that all data is accurate.
If you have suggestions for improving this survey (including new entrants in the market), please contact one of the authors.
The 2023 Milliman Long Term Care Insurance Survey, published in the July issue of Broker World magazine, was the 25th consecutive annual review of long term care insurance (LTCI) published by Broker World magazine. It analyzed product sales, reported sales distributions, and detailed insurer and product characteristics.
From 2006-2009, Broker World magazine published separate group LTCI surveys, but discontinued those surveys when the availability of group LTCI policies shrank. In 2011, Broker World magazine began this August annual analysis of worksite (“WS”) sales to complement the July overall market analysis.
The WS market consists of individual policies and group certificates (“policies” comprises both henceforth) sold with employer support, such as permitting on-site solicitation and/or payroll deduction. If a business owner buys a policy for herself and pays for it through her business, participants likely would not report her policy as a WS policy because it was not part of a WS group. If an employer sponsors LTC/LTCI educational meetings, with employees pursuing any interest in LTCI off-site, sales would likely not be reported as WS sales.
We limit our analysis to US sales and exclude “combination” products, except where specifically indicated. (Combination products pay meaningful life insurance, annuity, or disability income benefits in addition to LTCI.)
As reported in Market Perspective, the bulk of worksite sales that cover support with activities of daily living (ADLs) or cognitive impairment do not qualify as LTCI under section 7702(B) and are not covered in this survey (except as specifically mentioned).
About the Survey Participants Seven participants (Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian Life, New York Life, Northwestern, and Thrivent) contributed broadly to stand-alone sales distributions reported herein. Total 2022 sales data includes one additional contributor (LifeSecure) and 2022 inforce data includes two additional contributors (LifeSecure and CalPERS).
Our survey includes stand-alone WS sales and statistical distributions from participants National Guardian Life, New York Life, and Northwestern, and WS sales data from contributor LifeSecure.
The following eleven insurers participated in our combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual (Northwestern), OneAmerica, Pacific Life (2021 survey only), Securian, Trustmark and United of Omaha.
Comparisons of sales distributions We compare WS sales to individual LTCI policies that are not WS policies (NWS) and to total sales (Total).
Our WS stand-alone statistical distributions can vary significantly from year-to-year because insurers focusing on particular WS markets may be over- or under-represented. As has been the case for several years, our worksite sales distributions are dominated by executive sales. Carriers that provided 2022 distributions had an average worksite annual premium of $2,565, excluding FPOs, whereas the insurers that provided sales, but not distributions, had an average worksite premium of $1,876 annually. We believe this difference is narrower than in the past several years because of the inclusion of delayed Washington sales in our 2022 WS data.
Highlights from This Year’s Survey As explained in the July issue, a large number of 2021 applications were delayed by insurer backlog in 2021, eventually being issued in 2022. We successfully worked with most participants to reassign cases to 2021 so we could isolate the boost in 2021 sales driven by the Washington Cares Fund (WCF) exemption rules. Nonetheless, our total sales distributions are still somewhat impacted by delayed 2021 sales in the state of Washington.
Reassigning those policies was a lot of work for participants, so we chose not to reassign corresponding worksite policies to 2021. Thus, while our total distributions are largely adjusted for such lag, our WS distributions are not adjusted for such lag. Our NWS distributions are also not adjusted for such lag, because we calculated NWS distributions by subtracting unadjusted WS sales from unadjusted total sales. Readers should keep in mind that some results may be meaningfully different next year when all data will be on the same basis.
Table 1 shows the number of sales and premium in the total market and in the worksite market both nationally and in Washington for years 2020 to 2022. Including NAIC data for non-participants, it shows that Washington accounted for 75 percent of reported stand-alone LTCI policies sold in 2021 (an estimated 35 percent of premium) and 54 percent of combination life/LTCI policies (21 percent of premium).
Stand-alone worksite 2022 sales receded significantly from their higher, Washington-impacted 2021 sales. Participants reported worksite sales of 2,213 lives and $8.7 million in premium, compared to (for same companies) pandemic-influenced 2020 sales of 2,124 lives and $7.1 million of premium. Transamerica, which produced more 2020 worksite sales than all our participants combined, stopped selling in the first half of 2021 and is not included in the prior sentence. Thus, our participants appear to have, at best, absorbed a small portion of Transamerica’s share of the worksite market. As discussed in Market Perspective, many worksite sales with coverage for ADL-deficiency and cognitive impairment shifted to products that do not qualify as LTCI under section 7702(B).
As shown in Table 1, stand-alone WS sales (including Transamerica) dropped significantly from 2020 to 2022, but combo worksite reported sales increased by 13 percent (number of coverages) and 49 percent (annualized premium).
Worksite sales contributed eight percent of participants’ stand-alone sales in 2022 and seven percent of stand-alone annualized premium, as explained in the discussion of Table 3. Table 1 also shows that Washington accounted for 15 percent of the reported 2022 worksite cases and six percent of the worksite premium, indicating a low average premium for Washington sales compared to National. Washington’s higher market share in terms of policies is an indicator that our stand-alone worksite sales include many delayed 2021 sales. Our numbers reflect a significant drop in stand-alone LTCI sales in the worksite, which would be even greater had we adjusted worksite sales for the Washington sales lag.
As reported in our July issue, the number of 2021 Washington stand-alone LTCI sales was approximately 90 times the 2020 Washington sales. The ratio varies significantly between worksite insurers (483) and individual insurers (26).
In the combo market, worksite sales accounted for 39 percent of participants’ reported coverages sold and eight percent of annualized premium. Life/LTCI combo insurers sold 89 times as many coverages in Washington in 2021 than in 2020. The ratio also varies significantly between worksite insurers (578) and individual insurers (21). We include here some WS policies that qualified for exemption from the WCF tax even though they do not qualify under section 7702(B), which largely explains different results than some other reports. We have a good-sized sample of combo insurers, but a lower percentage of industry sales than in the stand-alone market.
MARKET PERSPECTIVE There are three segments of the WS market. A single WS case may involve different segments for different employee classes.
In “core” (also known as “core/buy-up”) programs, employers pay for a small amount of coverage for generally a large number of employees. Employees can buy more coverage. “Core” programs generally have low average ages, short benefit periods, low daily maximum benefits and a small percentage of spouses insured.
In “carve-out” programs, employers pay for robust coverage for key executives and usually their spouses. Generally, executives can buy more coverage for themselves or spouses. Compared to “core” programs, a higher percentage of insureds are married, more spouses buy coverage, the age distribution is older and average premium is higher.
In “voluntary” programs, employers pay none of the cost. The typical coverage is more robust than “core” programs, but less robust than “carve-out” programs. Voluntary programs tend to be most weighted toward female purchasers.
National Guardian, New York Life, and Northwestern write mostly executive carve-out programs and are the only insurers that provided statistical distributions; therefore, our data is heavily weighted to the executive carve-out market. If an employer purchases coverage for only one or two employees, the insurer may not recognize the case as executive carve-out, in which case we would under-report executive carve-out sales.
Because of tax savings, small executive carve-out issue dates are weighted toward the end of the year. On the other hand, large voluntary cases are traditionally weighted toward fall enrollments with January 1 effective dates. Large voluntary cases are probably more evenly distributed through the year than in the past, but differences remain.
Carrier and product shift: Last year, we noted that the future of the non-executive carve-out LTCI market was unpredictable with Transamerica’s departure. This year’s decline in the stand-alone WS market was not surprising.
WS programs have gravitated toward products that include life insurance, which is viewed as a more immediate potential need by young employees with families. The possibility of guaranteed issue also draws employee benefit advisors and employers to such products. Such products can allow 100 to 300 percent of the death benefit to be used for “chronic illness” (defined in terms of ADLs and cognitive impairment), typically using up to four percent of the death benefit each month. Alternatively, they can allow 100 to 200 percent of the death benefit to be used, restoring used death benefit each month so beneficiaries will receive the full death benefit.
These products do not qualify as LTCI under section 7702(B). As they have a fixed chronic illness benefit, the purchasing power of the coverage typically deteriorates over time. For example, if a 30-year-old employee buys a $100,000 death benefit, she will have a $4,000 maximum monthly benefit for chronic illness (assuming the benefit features described above). That $4,000 benefit would cover a much higher percentage of her cost of care if she needed care in the next few years compared to if she needs care 50 years from now.
Washington Cares Fund: Washington state’s “Washington Cares Fund” (WCF) imposes a 0.58 percent employee-paid payroll tax to fund a $36,500 lifetime pool (intended to inflate according to the Washington consumer price index) for care, as defined in the Revised Code of Washington 50B.04, received in Washington. People who purchased private stand-alone or combination LTCI by November 1, 2021 could file to be exempt from the tax. WCF received approximately 484,000 applications for exemption.1
Other states are interested in state-run LTCI programs. Examples include:
California: A task force identified alternative programs which are being priced in 2023. Recommendations will be made to the legislature for possible 2024 legislation.
New York SB 9082 did not pass in 2022 and no legislation was proposed in NY’s 2023 legislative session. However, Governor Hochul issued an executive order in November 2022 citing her “vision of a long-term care system that is accessible, effective, and affordable.”2
In Minnesota, bills for a state LTCI program have been introduced twice. The state has commissioned a study to be produced in 2023 to explore alternatives.
Pricing and Underwriting Considerations: Most people interpret Title VII of the 1964 Civil Rights Act to require that employer-involved LTCI programs use unisex pricing if the employer has had at least 15 employees for at least 20 weeks either in the current or previous year. Some states apply similar laws to employers with fewer employees. The expense of separate pricing, marketing and administration discourages insurers from serving both the WS and NWS markets.
Moreover, insurers fear anti-selection. Because women have higher expected future claims, unisex pricing saves women money compared to gender-distinct NWS pricing, whereas men pay much more with unisex pricing than with gender-distinct pricing. Insurers may vary pricing based on the employees’ gender distribution.
Insurers also fear health anti-selection (less-healthy people buying, while healthier people do not buy). Insurers are more vulnerable to health- or gender-anti-selection if the group has a large portion of young or less affluent employees as this group is generally less likely to buy LTCI. When the coverage has a life insurance component, more employees are likely to buy, which can help reduce the insurer’s anti-selection concerns.
Furthermore, because WS programs rarely offer “preferred health” discounts, healthy couples may pay more for WS coverage than for corresponding NWS coverage.
To control risk, most insurers will not accept a voluntary WS program if there are fewer than 100 employees. However, one insurer (which offers no health concessions) will accept voluntary LTCI programs with as few as 2 to 5 (varies by jurisdiction) employees buying.
Because of tax advantages when an employer pays the premium, a more expensive WS product can still produce after-tax savings compared to a cheaper NWS policy. The specter of future tax increases enhances the attractiveness of employer-paid premium.
Availability of coverage: As few people younger than age 40 buy stand-alone LTCI, some insurers have raised their minimum issue age to avoid anti-selection and to reduce exposure to extremely long claims. Such age restrictions can discourage employers from introducing a program, especially a carve-out program if they have executives or spouses too young to be covered.
With increased remote work, more employers have employees stretched across multiple jurisdictions and eligible non-household relatives might live anywhere. But insurers may not offer a product in jurisdictions with difficult laws, regulations or practices, such as slow policy form approval. So, it can be difficult to find a product which can cover everyone unless LTCI is sold on a group policy form and the employer does not have individuals in extra-territorial states.
One contributor no longer offers WS LTCI to non-household relatives. Reduced availability for such relatives does not have much impact on sales, because typically a small percentage (about one percent of 2022 sales) of WS buyers are not an employee or partner. If a program does help elder relatives, it is still not likely to meaningfully address the negative impact of employees being caregivers.
Prior to gender-distinct pricing, an executive carve-out for two partners of a company with more than 15 employees could have been serviced by any LTCI company, but now it is hard to find a carrier that offers unisex pricing under such circumstances. Such executives may buy policies with gender-distinct pricing either because they are unaware of the requirement under Title VII of 1964 Civil Rights Act; they may disagree with the interpretation that such policies should have unisex pricing to avoid the risk of a civil rights complaint; etc.
Some employee benefit brokers are reluctant to embrace LTCI because of declinations, the effort of enrollment, certification requirements, their personal lack of expertise, etc. WS sales gain from LTCI specialists forming relationships with employee benefit brokers.
Support for Employees who are Caregivers: Various programs offer LTC-related services to employees and their families. Regardless of whether the employee is insured or the relative is insurable, they may be able to access information, advice, services, and products that make caregiving more efficient, more effective, safer, and less expensive. Enabling employees and their families to have better LTC experiences and to use more (not necessarily 100 percent) commercial care should boost productivity at work. Some of these programs are packaged with WS LTCI.
STATISTICAL ANALYSIS As mentioned earlier, insurers’ sales distributions can vary greatly based on the submarket they serve (for example, in the WS market: core, voluntary, or carve-out). Therefore, in addition to fundamental changes in the industry, distributions may vary significantly from year to year due to a change in participating insurers, distribution within an insurer, and market share among insurers. Policies in the carve-out market are designed similarly to those in the NWS market. Our sales distributions reflect only stand-alone LTCI. Two insurers reported their number of new employer cases as well as the number of new worksite sales. Combined, they averaged 7 applications per new employer case, which seems to confirm the executive carve-out concentration in our data.
The aggregate sales section includes estimates for 2021 and 2020 to reflect a more accurate picture of the industry. Subsequent sections do not include sales estimates.
Aggregate Sales Table 1 shows the number of sales and premium in the total market and in the worksite market both nationally and in Washington for years 2020 to 2022. Table 1 spotlights the impact of Washington on 2021 sales and the drop in worksite sales in 2022.
Last year, to provide a clearer view of what happened in Washington in 2021, we estimated 2020 and 2021 sales from non-participants. A lot of 2021 sales, particularly worksite sales, were made by non-participants. However, the non-participant with the bulk of the 2021 sales stopping selling in mid-2021. In 2022, we did not estimate sales of non-participants, as our general observations of the market would be unchanged.
Table 2 shows historical WS sales over a longer period of time, including some estimates based on our review of NAIC data. It shows overall average WS premium for all carriers that reported sales compared to the average WS premium for the participants who contributed statistical data beyond sales. As shown in Table 2, our WS statistics likely represented the broad WS market reasonably until 2017 (the WS average premium for survey participants was similar to the total average premium before 2017). Average premiums plummeted last year because of the WA sales. We believe the full survey participant average premium was lowered by delayed Washington policies.
Table 3 shows WS sales as a percentage of total LTCI sales. As noted earlier, the WS percentage declined in 2022 due to an insurer dropping out of the market. The 2022 percentages would be significantly lower if we had removed the sales pushed into 2022 by the flood of 2021 applications.
Market Share Table 4 shows the insurers’ reported WS sales, including FPOs and additions to worksite cases issued in prior years. Excluding FPOs, New York Life would have been in the lead, followed by LifeSecure.
We also examined the distribution of new insureds by jurisdiction for both the total market and the WS market. The WS market share of five states (AK, IA, ND, VA and WA) was 50 percent or more greater than their overall market share (e.g., if they had a two percent overall market share, they had at least a three percent market share in WS). In 18 jurisdictions, the market share of total sales was at least 50 percent greater than the WS market share, suggesting that there may be opportunity for WS sales in these jurisdictions: AL, CO, IN, KS, ME, MD, MA, MI, MO, NE, NH, NM, PA, SC, TX, UT, VT, and WI. In five jurisdictions, our participants had no stand-alone WS sales at all (DC, RI, WV, WY, and Puerto Rico).
Average Premium Per Buyer Table 5 shows the average premium per new insured (NB Insured) and per buying unit (a couple comprise a single buying unit). For these two average sizes to be comparable, we must include only insurers which report sales for couples. The average premium per new insured including all insurers that reported sales is $3,556.
As always, the average premium per buying unit (a couple comprise a single buying unit) is higher because there are fewer buying units than insureds. Normally, the increase in average premium per buying unit compared to per insured is lower for WS sales, because more WS buyers are single and because spouses are less likely to buy in the WS. However, in the carveout market, more buyers are married and spouses are more likely to buy.
Issue Age In reviewing the balance of the statistical presentations, we urge you to be selective in how you use the data because it is not representative of the entire WS market as explained above.
Table 6 shows that the average age increased 6 to 7 years for both the NWS market and the WS market, which was generally expected due the influence of 2021 Washington sales.
Table 7 shows how much older the average NWS buyer has been compared to the average WS buyer.
Table 8 displays the relative age distribution of workers ages 16+ vs. the age distribution of purchasers in the WS market. It also shows the age distribution of adults 20-79 compared to the age distribution of purchasers in the NWS market. If the percentage of sales in a particular age group is higher than the percentage of population in that age group, we can conclude either that LTCI is more appealing to that age group or that the industry gets in front of that age group more. For whichever reason, the industry is particularly effective with ages 40-49 in the WS market. In the NWS market, the industry is particularly effective for ages 50-69.
Rating Classification Most WS sales are in the “best” underwriting class (see Table 9) because there generally is only one underwriting class. Insurers often do not get enough information in WS to determine whether a “preferred health” discount could be granted and use the additional revenue (from not having a “preferred health” discount) to fund extra cost resulting from gender or health anti-selection. Carve-out programs are more likely to offer a “preferred” discount, which means a higher percentage of carve-out policies are issued in the second-best underwriting class. The percentage of policies issued in the best underwriting class soared in the NWS market in 2021 because younger and healthier buyers were drawn to LTCI in WA.
Benefit Period The WS average benefit period is low for core/buy-up programs and somewhat low for voluntary programs. Executive carve-out programs sometimes have longer benefit periods than the NWS market. In 2022, the average benefit period returned to pre-2021 levels. The NWS market had an average benefit period of 3.70 years compared to 3.76 in 2020. The WS market had an average benefit period of 3.44 compared to 3.54 in 2020.
The difference in benefit periods between the markets is larger than these statistics indicate, because these statistics ignore Shared Care (the WS market issues much less Shared Care).
Table 11 shows corresponding data back to 2014. As noted elsewhere, this data can jump around based on which insurers provide such detail and whether large core/buy-up cases are written in a particular year.
Maximum Monthly Benefit In 2020, the average initial monthly maximum was about nine percent lower in the WS market than in the NWS market. In 2021, the difference tripled to 27 percent lower in the WS market. To calculate the average initial monthly maximum, we presume an average size in each size range. The $2,100/month we assume for the smallest size range seems to overstate dramatically in 2021 as many people opted for the minimum $1,500/month.
The Total Market average initial monthly maximum was the highest we have seen since 2015 partly due to a shift in distribution away from the WS market (see Table 13). The WS initial monthly maximum varies more over time than the whole market because of participant changes and how many core/buy-up plans were sold in a particular year.
Benefit Increase Features As shown in Table 14, 9.1 percent of 2022 WS sales had compounding of three percent or higher, compared to 2.8 percent in 2021 (and 5.6 percent in 2020). Of the 2022 WS sales, 24 percent had no increase feature and 63 percent had a FPO feature.
In the NWS market, 29.2 percent had three percent or higher compounding compared to 24.5 percent in 2021 (and a 35.5 percent in 2020).
Future Protection Based on a $27/hour cost for non-professional personal care at home ($27 is the median cost according to Genworth’s 2021 Cost of Care Survey), the average WS initial maximum daily benefit of $145 would cover 5.4 hours of such care per day at issue, whereas the typical NWS initial daily maximum of $169 would cover 6.2 hours of such care per day, as shown in Table 15.
The number of future home care hours that could be covered depends upon when care is needed (we have assumed age 80), the home care cost inflation rate between now (age 46 for WS and 58 for NWS) and age 80 (we have calculated with two, three, four, five and six percent inflation), and the benefit increases provided by the LTCI coverage between now and age 80.
Table 15 shows calculations for three different assumptions relative to benefit increase features:
The first line presumes that no benefit increases occur (either sold without any benefit increase feature or no FPOs were exercised).
The second line reflects the average benefit increase design using the methodology reported in the July article, except it assumes that 40 percent of FPOs are elected (intended to be indicative of “positive” election FPOs, in which the increase occurs only if the client elects it) and provide five percent compounding.
The third line is like the second line except it assumes 90 percent of FPOs are elected (intended to be indicative of “negative” election FPOs, in which the increase occurs unless the client rejects it). It also assumes the FPOs reflect five percent compounding.
Table 15 indicates that:
Without benefit increases, purchasing power deteriorates significantly, particularly for the WS purchaser as younger buyers have more years of future inflation prior to claim onset. For example, with a flat benefit, the number of covered hours of home care at age 80 drops to 2.0 hours for the average WS purchase age if there is three percent inflation and fewer than 2 hours if inflation is higher. The average NWS buyer would have 3.3 hours of care (rather than 2 hours) at age 80 if they had no benefit increases and inflation was three percent because the average NWS buys a larger daily benefit and is older.
The “composite” (average) benefit increase design assuming that 40 percent of FPO offers are exercised preserves purchasing power better than when no increases are assumed. The average WS buyer gains buying power over time if the inflation rate is two percent, being able to pay for 6.7 hours at age 80. But if the inflation rate is four percent, this drops approximately in half. The average NWS buyer does better because of a higher initial maximum daily benefit and a higher issue age.
Assuming that 90 percent of FPO offers are exercised, this buyer would have at least as much coverage at age 80 as at issue if the inflation rate is less than four percent. The average NWS buyer has increasing purchasing power until inflation averages more than 3.3 percent.
Table 15 underscores the importance of considering future purchasing power when buying LTCI. Please note:
The average 2022 WS buyer was 12 years younger at issue than the average 2022 NWS buyer, hence has 12 more years of inflation and benefit increases in the above table. The actual inflation rate to age 80 is not likely to be the same for today’s 46-year-olds as for today’s 58-year-olds.
Individual results vary significantly based on issue age, initial maximum monthly benefit, and benefit increase feature, as well as the inflation rate and the age at which the need for care occurs.
Between the median age of starting to need care (about age 83) and the median age of needing care (about age 85), more purchasing power could be gained or lost.
Table 15 does not reflect coverage for professional home care or facility care. According to the 2021 Genworth study, the average nursing home private room cost is $297/day, which is currently comparable to 11 hours of non-professional home care. However, the inflation rate for facility costs is likely to differ from the inflation rate for home care. From 2004-2021, Genworth’s studies showed the following compound growth rates: private room in a nursing home (3.0 percent), assisted living facility (3.8 percent), home health aide (2.2percent), and home care homemaker (2.6 percent).
Table 15 could be distorted by simplifications in our calculations. For example, we assumed that the FPO election rate does not vary by age, size of policy or market and that everyone buys a home care benefit equal to the average facility benefit.
FPO election rates might be different for policies purchased in 2021. How likely is it that 2021’s WA buyers will exercise FPOs?
Partnership Program Background When someone applies to Medicaid for long-term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (with some policies, IN and NY disregard all assets). Partnership programs exist in 44 jurisdictions (all but AK, DC, HI, MA, MS, UT, and VT), but MA has a similar program (MassHealth). The first four states to develop Partnerships (CA, CT, IN and NY) have different rules, some of which have become a hindrance to sales. We are not aware of a Partnership-qualified WS LTCI product in those four states, which is unfortunate because the WS market serves many people who could benefit from Partnership.
To qualify for a state Partnership program, a policy must have a sufficiently robust benefit increase feature. Many jurisdictions have lowered the minimum Partnership-eligible compounding benefit inflation rate to one percent. To facilitate Partnership sales in such jurisdictions, an insurer could lower its minimum size by 1/3 (e.g., from $1,500 to $1,000) if one percent compounding is included in a core program. The revenue from the core program would typically increase. The premium would be more level by issue age, shifting risk to younger ages which can be preferable for the insurer in a core program.
Jurisdictional Distribution The 2023 Milliman Long Term Care Survey includes a chart of the market share of each US jurisdiction relative to the total, WS and NWS markets, and the Partnership percentage by state. This chart indicates where relative opportunity may exist to grow LTCI sales.
Elimination Period More than 90 percent of the NWS market buys 90-day elimination periods (EPs). For that reason, many WS programs offer only a 90-day EP.
Table 16 shows distribution by EP and how many policies had a 0-day home care feature and a longer facility EP and how many policies had a calendar-day EP (as opposed to a service-day EP). We have reflected that all LifeSecure policies are 90-day EP with a calendar-day definition. Policies which have 0-day home care EP and define their EP as a service-day EP operate almost identically to a calendar-day EP, because people in facilities get daily care.
Gender Distribution and Sales to Couples and Relatives Insurers began gender-distinct LTCI pricing in 2013, but as explained above, unisex pricing continues in the WS market.
In the NWS market, the 2013-2015 percentages of females were high as insurers that still offered unisex pricing attracted single females. The next 5 years, the percentage of female buyers in the NWS was stable, fluctuating from 54.3 to 54.9 percent. In 2021, women constituted 50.5 percent of the US age 20-79 population3, but in 2021 the percentage of females dipped below 50 percent in both the WS and NWS markets because of the higher number of males purchasing coverage in WA.
In the WS market, the high percentage of female WS buyers from 2015-2018 suggests that women were particularly attracted to WS LTCI (presumably because of unisex pricing). To the degree that our more recent WS data is over-weighted to executive carve-out programs, it reflects less of the gender anti-selection that likely still exists. Although most executives are male, executive ranks are becoming more gender-balanced and many executive carve-out programs cover spouses. Women make up 47 percent of workers4 but accounted for 55 percent of our reported 2022 WS sales.
Table 18 digs deeper, exploring the differences between the WS and NWS markets in single female, couples and Shared Care sales. The percentage of NWS insureds who are female (49.9 percent) spotlights our statistical distribution difficulties this year. Insurers that reallocated sales from 2022 to 2021 probably moved a high percentage of males from total sales. As the worksite number of males was not adjusted, our method subtracted an unadjusted (high) number of WS males from an adjusted (low) number of total males, producing a misleading high number of NWS males, which explains our low 49.9 percent for females.
Our WS data had more single buyers, but a lower percentage of single buyers were female.
Slightly more than half the couples in the WS market insured both partners; slightly fewer than half of the couples in the NWS market did so.
Shared Care is less often offered in a WS program.
Our limited data with regard to relatives who buy shows that two spouses are insured for every three employees. That’s a high percentage reflective of executive carve-out data. Only about one percent of purchasers are relatives other than the employees and employees’ spouses.
Type of Home Care Coverage Table 19 summarizes sales by type of home care coverage. Historically, the WS market sold few policies with a home care maximum equal to the facility maximum. However, with increasing emphasis on home care and simplicity, that difference faded.
Table 19 also shows that monthly determination dominates both markets.
Because some insurers build these features into products automatically, we are able to include data from an insurer which did not provide sales distributions.
Many WS products embed a “partial cash alternative” feature (which allow claimants, in lieu of any other benefit that month, to use approximately 1/3 of their benefit for whatever purpose they wish, with the balance extending the benefit period) or a small informal care benefit.
Other Features Table 20 shows that almost all Return of Premium (ROP) features were embedded (automatically included) and phased out before death would be likely. ROP with expiring death benefits may provide an inexpensive way to encourage more young people to buy LTCI but does not address the buyer’s concern (what if I keep paying all my life, then die without qualifying for benefits?).
Table 21 shows lower Joint Waiver of Premium and Survivorship sales to couples in the WS market than in the NWS market, mostly due to differences in distribution by carrier. Some products automatically provide Joint Waiver of Premium if a couple buys identical coverage or if a couple buys Shared Care. Employers sometimes are disinclined to add an optional couples’ feature because they are already contributing more money to cover a married employee plus that employee’s spouse than the cost for a single employee the same age.
CLOSING We thank insurance company staff for submitting the data and responding to questions promptly. We also thank Sophia Fosdick and Quentin Clemens of Milliman for managing the data expertly.
We reviewed data for reasonableness. Nonetheless, we cannot assure that all data is accurate. If you have suggestions for improving this survey, please contact one of the authors.
The 2023 Milliman Long Term Care Insurance Survey is the 25th consecutive annual review of stand-alone long-term care insurance (LTCI) published by Broker World magazine. It analyzes the marketplace, reports sales distributions, and describes available products.
More discussion of worksite sales, including a comparison of worksite sales distributions vs. non-worksite sales distributions will be in Broker World magazine’s August issue.
Unless otherwise indicated, references are solely to U.S. stand-alone LTCI sales, excluding exercised future purchase options (FPOs) or other changes to existing coverage. “Stand-alone” refers to LTCI policies that do not include death benefits (other than returning premiums upon death or waiving a surviving spouse’s premiums) or annuity or disability income benefits. Where referenced, “combo” or “combination” products provide LTCI combined with life insurance or annuity coverage. “Linked benefit” policies are combo policies which can allow more than the death benefit or annuity account value to be used as LTCI.
All references to sales in terms of “premium” refer to “annualized” premium (1 x annual; 2 x semi-annual; 4 x quarterly; 12 x monthly), even if only one monthly premium was received before year-end. All references to “Washington” or “WA” refer to the state of Washington. “WCF” refers to the “WA Cares Fund,” explained in the Market Perspective section.
Highlights from this year’s survey
As reported last year, the WCF stimulated tremendous market demand in the state of Washington, causing sales distributions to vary greatly from recent history. Although the industry largely stopped accepting Washington applications in August 2021, a backlog resulted in some policies being issued in 2022. To get a better understanding of the impact of the backlog, we asked insurers to reclassify 2022 sales to 2021 if they were issued in 2022 due to the unusual lag. For the purpose of compiling results for this article, figures that display industry sales levels reflect our adjustments because of the backlog. However, all insurer-specific sales data ignores any backlog adjustment. In the sales distributions section of our report, some insurers’ data reflect the sales backlog (i.e., 2021 sales that lagged into 2022) while other insurers were able to remove them. For that reason, we generally anticipate that 2022 sales distributions are likely to differ from 2023 sales distributions.
Participants Seven insurers (Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian Life, New York Life, Northwestern, and Thrivent) contributed broadly to stand-alone sales distributions reported herein. Total 2022 sales data includes one additional insurer and 2022 inforce data includes two additional organizations.
Our worksite sales distributions do not reflect low-price worksite programs; however, the gap in average premiums was smaller than usual. Carriers that provided 2022 distributions had an average worksite annual premium of $2,565, whereas the insurers that provided sales, but not distributions, had an average worksite premium of $1,876 annually.
In 2021, we collected data on combination sales (life insurance with LTCI or Chronic Illness benefits) for the first time to evaluate the impact of the WCF exemption on sales. This year, we did so again. The following eleven insurers contributed to our combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual (Northwestern), OneAmerica, Pacific Life (2021 data only), Securian, Trustmark and United of Omaha.
Sales Summary
We estimate total stand-alone LTCI annualized new premium sales of nearly $124 million in 2022 (including exercised FPOs except FPOs for insurers no longer selling LTCI and counting 10 percent of single premium), compared to $200 million in 2021 (same basis). The 2021 sales are influenced by the higher Washington sales and include estimated sales for one insurer for which we did not estimate sales this year. In addition, there was a $7 million drop in 2022 in new premium from FPOs.
Outside-of-Washington sales trends are likely to be more reflective of the future. Our participants’ outside-of-Washington 2022 premium (including FPOs) was eight percent higher than their outside-of-Washington 2021 new premium. However, compared to 2020 sales including insurers which have left the market, the sales dropped 23 percent. The continuing insurers have been able to maintain their own sales levels (2022 premium was 99 percent of 2020) but not replace the sales of departing insurers. On a lives basis, the 2022 sales data was roughly 88 percent of 2020 for continuing insurers (versus the 99 percent on a premium basis), reflective of the higher prices of today’s stand-alone LTCI policies.
Worksite sales receded significantly from their higher, Washington-impacted 2021 sales. All participants reported worksite sales of 2,213 lives and $8.7 million in premium, compared to pandemic-influenced 2020 sales of 2,124 lives and $7.2 million of premium. Transamerica, which produced more 2020 worksite sales than all our participants combined, stopped selling in the first half of 2021, depressing product availability, and is not included in the sales in this paragraph. Thus, our participants did not absorb Transamerica’s share of the worksite market.
Northwestern led in annualized new premium including FPO elections, selling 13 percent more than the #2 and #3 insurers combined (Mutual of Omaha and New York Life). Northwestern edged ahead of Mutual of Omaha in annualized premium from new policies although Mutual of Omaha still sold more new policies.
Reflecting nine entities’ data, the inforce number of cases dropped 1.4 percent while annualized premium increased 3.5 percent. Inforce premium rises due to sales, price increases, and benefit increases (including FPOs), and falls from lapses, reductions in coverage, deaths, and shifts to paid-up status. The number of people with stand-alone coverage increased through 2014, but, as shown in Table 1, has decreased annually since then except for the 2021 aberration. However, the inforce premium has increased each year because of inforce price increases and higher prices for new policies.
Collectively, eight participants paid five percent more in claims in 2022 than in 2021. Overall, the stand-alone LTCI industry incurred $13.6 billion in claims in 2021 based on companies’ statutory annual filings, a 5.4 percent increase over 2020, which raises the running total of incurred claims since 1991 to $180.9 billion (2021 claims of $13.6 billion plus total of $167.3 billion from our prior year’s article). Most of these claims were incurred by insurers that no longer sell LTCI.
About the Survey This article is arranged in the following sections:
Highlights provides a high-level view of results.
Market Perspective provides insights into the LTCI market.
Claims presents industry-level claims data.
Sales Statistical Analysis presents industry-level sales distributions reflecting data from 8 insurers.
Partnership Programs discusses the impact of the state partnerships for LTCI.
ONLY AVAILABLE AT WWW.BROKERWORLDMAG.COM:
Product Exhibit shows, for 6 insurers: financial ratings, LTCI sales and inforce policies, and product details.
Product Exhibit Details, a row-by-row definition of the product exhibit entries, with some commentary.
Premium Exhibit shows lifetime annual premiums for each insurer’s most common underwriting class, for issue ages 40, 50, 60, and 70 for single females, single males, and female/male couples (assuming both buy at the same age), based on $100 per day (or closest equivalent weekly or monthly) benefit, 90-day facility and most common home care elimination period, three-year and five-year benefit periods or $100,000 and $200,000 maximum lifetime buckets, with and without Shared Care and with flat benefits or automatic three or five percent annual compound benefit increases for life. Worksite premiums do not reflect any worksite-specific discount, though some carriers offer this.
Premium Adjustments (from our Premium Exhibit prices) by underwriting class for each participant.
Distribution by underwriting class for each participant. Depending upon the product shown for an insurer in the Product Exhibit, we sometimes adjust that insurer’s underwriting distribution to provide readers a better expectation of likely results if they submit an application in the coming year and to line up with the prices we display. For example, if the Product Exhibit shows only a new product which has only one underwriting class (hence one price), but the insurer’s data partly or solely reflect an older product with three underwriting classifications, we might choose to show “100 percent” in their best (only) underwriting class.
State-by-state results show the percentage of sales by state, average premium by state and percentage of policies qualifying for Partnership by state.
MARKET PERSPECTIVE (more detail in subsequent parts of the article) Washington State’s “Washington Cares Fund” (WCF) stimulated tremendous demand for private LTCI from individuals and businesses in Washington in 2021. WCF imposes a 0.58 percent payroll tax to fund a $36,500 lifetime pool (intended to inflate according to the Washington consumer price index) for care, as defined in the Revised Code of Washington 50B.04, received in Washington. People who purchased private stand-alone or combination LTCI by November 1, 2021 could file to be exempt from the tax. WCF received approximately 484,000 applications for exemption.1
Partly because the tax applies to all earned income, 2021 LTCI sales in Washington soared to unprecedented levels. Insurers quickly became backlogged with applications and were concerned about early lapses as the law provided a permanent WCF exemption based on only a one-time attestation. Insurers reduced design flexibility, and then discontinued sales in Washington before the November 1 deadline.
(Note: The WCF continues to contemplate further program changes. In particular, a future change may require retention of private LTCI coverage to maintain exemption from the WCF tax and some care outside of Washington might be covered.)
Last year, we estimated that Washington accounted for 75 percent of stand-alone LTCI policies sold in 2021. Of combination life/LTCI business with on-going premium (i.e., excluding single premium), we estimate Washington accounted for 60 percent of policies sold in 2021 but only 20 percent of premium. This year, even after adjusting with data from the NAIC and removing FPOs, the stand-alone policy percentage remains 75 percent. As shown in Table 3, the percentage of 2021 combo policies sold in WA is revised from 60 to 54 percent because we added a carrier with a relatively small percentage of its business in Washington.
Washington continued to account for a high percentage of business issued in 2022 because of delayed processing of third quarter 2021 applications. With participants’ help, we moved 76 percent of 2022 WA stand-alone policies issued (33 percent of premium) and 66 percent of 2022 WA combo policies (26 percent of premium) to 2021. Moving these policies increased 2021 Washington sales only by five percent (4 percent of premium).
(Note: Washington’s share on stand-alone LTCI premiums is generally a bit lower than its share by policy count. We believe that is partly because some insurers have higher prices in other states such as CA, FL, and NY.)
Table 2 reveals that the WCF exemption seems to have stimulated additional sales beginning in 2020, boosting Washington’s market share of stand-alone policies to three percent in 2020 compared to a steady 2.4 to 2.5 percent prior to 2020. Washington’s market share in 2022 returned close to pre-2021 levels on an adjusted basis, both with and without adjusting for the mix of insurers across years. This suggests that our adjusted Washington 2022 market share is at most slightly influenced by the WCF exemption, but we will continue to monitor in future surveys.
Last year, we reported that insurers (including estimates for insurers which did not report sales) sold 90 times as many stand-alone LTCI coverages in Washington in 2021 as in 2020. After reflecting re-classification from 2022 and reviewing the 2020 and 2021 NAIC LTCI Experience Reports, we conclude that the 2021 number of Washington stand-alone LTCI sales remained approximately 90 times 2020 Washington sales. The ratio varies significantly between the worksite (483) and individual markets (26).
Last year, we reported that Life/LTCI combo insurers also sold more than 90 times as many coverages in Washington in 2021 as in 2020. This year’s updated calculation found a similar 89 times the 2020 total. The ratio varies significantly between worksite (578) and individual insurers (21).
Combining both stand-alone and combo polices, 90 times as many coverages were sold in Washington in 2021 as in 2020 but only 12 times as much premium.
Compared to 2020, the 2022 number of Life/LTCi sales in Washington is high but the 2022 premium is low, suggesting that we did not reclassify all of the lag.
In its 2022 report (“The WA Cares Act: Impact on Long Term Care and Hybrid Life Sales”), LIMRA reported the following third- and fourth-quarter increases in WA production in 2021 compared to the same period the previous year.
As dramatic as the LIMRA data is, our data shows much larger increases in Washington sales in 2021. The difference is primarily attributable to our inclusion of insurers focused on the worksite market (including group insurance). There was a huge demand for LTCi-related programs from Washington’s employers. A second, much smaller reason is our re-characterization of delayed sales back to 2021.
Idaho and Oregon also were impacted by the WCF exemption. Because WCF has been amended to allow out-of-state residents who work in Washington to be exempt, those sales may be at higher risk of lapsing as out-of-state residents no longer need to have a qualifying LTCI policy to be exempt. Table 5 shows Idaho and Oregon market share for the past several years. Our Idaho data shows a doubling of sales in 2021, but nearly back to pre-2021 levels for 2022. Our participants’ Oregon sales show little impact. However, as noted above, our statistical distributions do not reflect the worksite insurers. We believe inclusion of their data could show an approximately 50 percent increase in OR in 2021.
LIMRA kindly shared some of its sales findings as shown in table 6 (with some columns we added based on their data). As you can see, linked-benefit policies (“LTC Extension of Benefits”) and stand-alone LTCI (“traditional LTCI”) accounted for 20.2 percent of the policies and 16.6 percent of the premium.
In terms of protecting people against the risk of needing LTC, the contributions of stand-alone LTCI and linked-benefit products compared to acceleration products are likely greater than one might guess from these sales results. Consider:
Linked-Benefit and Stand-alone LTCI policies have lower voluntary termination rates, hence are more likely to be available when care is needed.
Linked-Benefit and Stand-Alone LTCI policies often have benefits that increase over time to help maintain purchasing power. Conversely, the purchasing power of Chronic Illness (CI) and LTC Riders (ADB) dwindles over time. However, purchasing power is a combination of the initial benefit plus increases; a large flat benefit could be sufficient when care is needed.
According to LIMRA, 88 percent of the CI policies have benefits that are not fixed. The insured has to cover the time value of money until death or expected death and sometimes other factors such as foregone premiums.
People are most likely to make LTC-related claims against stand-alone LTCI (it is use-it-or-lose-it) and second-most-likely to do so against linked-benefit products (to access the extension of benefits). Those products are more often purchased with LTC coverage in mind. In contrast, it may be more attractive to wait for the death benefit of acceleration policies, especially if the death benefit would be discounted when accessed to cover a LTC need.
Washington sales influenced the characteristics of 2021 sales significantly, as we reported last year and can be seen in this year’s results. Our sales distributions for 2022 continue to be somewhat influenced by Washington sales due to the backlog of policies that were not issued until 2022. Although we removed some of those backlogged Washington sales from our statistical distributions, we were unable to remove all such sales.
The national placement rate of 58.2 percent in 2022 was lower than the 61.4 percent in 2021 (unusually high due to Washington sales) but 0.4 percent higher than the 57.8 percent placement rate in 2020, as well as 4.1 percent higher than 2021’s 54.1 percent placement rate outside Washington. Our 2022 data includes some delayed young Washington applicants with higher placement rates.
Higher placement ratios are critical to encourage financial advisors to mention LTCI to clients. The following opportunities can improve placement rates.
E-applications speed submission and reduce processing time, thus generally increasing placement.
Uploading medical records via human application program interface (API) also speeds processing time, generally improving placement.
Health pre-qualification effectively and efficiently decreases decline rates.
Education of distributors, such as drill-down questions in on-line underwriting guides, tends to improve placement.
Requiring cash with the application (CWA) led to about five percent more of the apps being placed according to our 2019 survey.
Improved messaging regarding the value of LTCI and of buying now (rather than in the future) typically improves the placement rate by attracting younger and healthier applicants.
Other states are considering state-run LTCI programs. Examples include:
During 2023, alternatives identified by a California task force will be priced and recommendations will be made to the legislature for possible 2024 legislation.
In New York, SB 9082 was submitted in 2022 and Governor Hochul issued an executive order in November 2022 citing her “vision of a long-term care system that is accessible, effective, and affordable.”2
Minnesota, which has twice had bills for a state LTCI program, intends to produce a report in 2023 regarding Minnesota’s options to finance LTC that will be provided to the legislature.
There is a proposal in Massachusetts to create a task force to consider alternatives.
Such programs will likely differ from Washington’s program in several respects. For example, draft laws and task force discussions indicate that future laws:
May not leave the window open for people to opt out by buying LTCI after the legislation has been signed.
May require that private LTCI policies remain in force to maintain exemption.
May narrow the range of private LTCI policies that qualify for exemption.
The FPO (future purchase option, a guaranteed, or a non-guaranteed board-approved, option, under specified conditions, to purchase additional coverage without demonstrating good health) election rate dropped from 78.2 percent in 2021 to 69.9 percent in 2022, the decrease being more than explained by one more entity reporting FPO elections in 2022. The same six insurers which reported 78.2 percent in 2021 reported 88.4 percent in 2022.
As both the additional coverage and unit price increase for FPOs as policies age, FPOs become increasingly expensive, even more so with inforce price increases. The high election rate reflects the effectiveness of annual (as opposed to triennial) negative-election FPOs and may reflect the importance of LTCI to policyholders. Negative-election FPOs activate automatically unless the client rejects them. Positive-election FPOs activate only if the client initiates a timely request. Considering such FPOs and other increased coverage provisions, we project a maximum benefit at age 80 of $310/day for an average 57-year-old purchaser in 2022, which is equivalent to an average 2.7 percent compounded benefit increase between 2022 and 2045. In 2020, the average 58-year-old purchaser anticipated an age 80 benefit (in 2042) of $305 (2.9 percent compounding). So, the average 2022 purchaser will have $5 more in coverage at age 80, despite facing 3 more years of inflation in the cost of care. This is the lowest effective rate of compounding that we have seen in the survey, yet inflation appears to be an increasing threat now. Purchasers may be disappointed if the purchasing power of their LTCI policies deteriorates over time.
Current premiums are much more stable than past premiums, partly because today’s premiums reflect much more conservative assumptions based on far more credible data as well as lower assumed investment yields. Two participants have never increased premiums on inforce policies and a third has had no increases on policies issued since 2003. None of the participants have raised rates on policies issued in 2016 or later. Even for new products, pricing changes are becoming rare. There have been no new prices (other than late state approvals) in the past two years. Nonetheless, financial advisors may presume new policies will face steep price increases, hence be reluctant to encourage clients to consider LTCI.
Linked benefit and other combination products’ coverage are attractive to consumers because if the insured never has a LTC claim, their beneficiary will receive a death benefit. They also are more likely to have indemnity benefits and guaranteed premiums and benefits.
However, such policies generally cost more than stand-alone LTCI without a return of premium feature (if there is comparable LTC coverage at age 85), although the difference may be less than in the past. Higher interest rates and competition appear to be driving linked-benefit premiums lower, which are also more available now with on-going premiums. Meanwhile, stand-alone LTCI new business prices have generally increased in recent years, especially for one-of-a-couple sales.
As explained above, stand-alone and linked-benefit products typically provide more LTC protection at age 85 than those combination policies which provide LTCI only through an accelerated death benefit.
All the insurers in our Product Exhibit offer coverage in all U.S. jurisdictions, except that two insurers do not offer policies in New York.
At the suggestion of a reader, we surveyed carriers regarding hospice provisions this year. Eight insurers responded.
Five insurers define “hospice services” as being within six months of expected death, while one insurer indicated that their definition varies between 6 and 12 months depending on jurisdiction. Two insurers use a more general definition (e.g., “persons who are in the last phases of life due to terminal illness”), which is more flexible and seems less likely to conflict with potential future changes in general usage or regulations.
All insurers cover hospice care at home. Two insurers cover hospice only as part of their home care benefits, six insurers cover hospice services in ALFs and nursing homes, and seven insurers cover hospice services in hospice facilities.
None of the insurers cover hospice services provided to the terminally ill person’s family.
Four insurers waive the elimination period (EP) for hospice services; the other four insurers require that the EP be satisfied prior to reimbursing for hospice care.
Of the four insurers that waive the EP for hospice services, one credits hospice days to the “non-hospice” EP if either the insurer or Medicare pays for such days. The other three do not do so.
CLAIMS Independent Third-Party Review (IR) is intended to help assure that LTCI claims are paid appropriately. Since 2009 (in some jurisdictions), if an insurer concludes that a claimant is not chronically ill as defined in the LTCI policy, the insurer must inform the claimant of his/her right to appeal to IR, which is binding on insurers.
In many states, IR is not effective, either because the law was not adopted or because regulators have not set up the required panel of independent reviewer organizations (IROs). Nonetheless, a claimant could ask an insurer to agree to IR.
The Product Exhibit shows that most participants extend IR beyond statutory requirements (e.g., to policies issued prior to the effective date of IR). Some insurers utilize IROs as part of the insurer’s internal appeal process.
A very small percentage of claims go to IR. Indeed, of seven insurers which provided claims information this year, at least three have never had a request for IR.
We are not aware of regulators who track IR results, but Steve LaPierre, President of LTCI Independent Eligibility Review Specialists, LLC (LTCIIERS), the largest IR organization, reports that the insurer’s decision was upheld 98 percent of the time in 2022.
For comparison, a National Nurses United study of CA acute health claims3 indicates that half of the denials referred to independent review were overturned. Acute health insurance and LTCI claims are denied for different reasons which likely explains much of the difference in the rate at which the insurers’ decisions are overturned.
The LTCI industry’s IR experience indicates that insurers, overall, are paying claims appropriately.
Eight participants reported 2022 claims. As some companies are not able to provide complete detailed data, some statistics reported below are more robust than others.
The eight insurers’ combined individual and multi-life claim payments were five percent higher than in 2021.
The LTCI industry has paid out benefits to policyholders far greater than indicated in the following statistics, because most claims are paid by insurers that do not currently sell LTCI.
LTCI claims paid by insurers no longer selling LTCI may differ significantly from the following statistics as their claimants are more likely to have facility-only coverage, be older, and/or have other different policy or demographic characteristics.
In Tables 7 and 8, one insurer, representing 17 percent of inception-to-date claims, was unable to report the number claims since inception and their distribution by venue. “Since inception” means since the insurer first started selling LTCI or as far back as they can report these results (for example, they may have changed claims administration systems and not be able to go all the way back to when they first processed claims).
Table 7 shows the total dollar and number of reported individual and multi-life (not group) LTCI claims. As noted above, total paid claims were up five percent.
Table 8 shows that, for insurers reporting claims data, claims shifted away from nursing homes to assisted living facilities (ALFs). Different insurers contributing data from one year to another and/or contributing differently makes it harder to identify trends. For example, we learned in 2021 that one insurer previously assigned all of a claimant’s benefits based on the venue in the claimant’s first month of claim. Their 2021 and 2022 data is based on the venue for each claim payment, pushing Table 8 toward nursing homes, which implies that the shift from NH to ALF since 2020 and prior years is greater than the table indicates.
In the distribution based on number of claims, a person who received care in more than one venue is counted once for each venue, but not double-counted in the total line. The average claimant is in 1.5 types of venues during the course of the claim; this does not recognize multiple providers within a single type of revenue (e.g., two nursing homes).
Five carriers reported open individual claims at year-end, averaging 70 percent of paid claims, the same as last year.
Table 9 shows average size individual claims since inception: that is, including older claims and reflecting all years of payment. Assisted Living Facility (ALF) claims and Home Care claims showed lower average sizes this year, related to the change in reporting mentioned above. Because 48 percent of claimants since inception have submitted claims from more than one type of venue, the average total claim might be expected to exceed the average claim paid for any particular venue. Individual ALF claims stand out as high each year (albeit not as much this year), probably because:
a) ALF claims appear to have a longer duration compared with other venues.
b) Nursing home costs are most likely to exceed the policy daily/monthly maximum, hence nursing home claims are most likely to understate the cost of care.
c) People who maximize the use of their maximum monthly benefits can generally spend as much in an ALF as in a nursing home.
d) Although some surveys report that on average ALFs cost about half as much as nursing homes, ALFs may have an extra charge for a memory unit or for levels of assistance that align more closely with nursing home care.
Several insurers extend ALF coverage to policies which originally did not include ALF coverage, providing policyholders with significant flexibility at the time of claim but contributing to the insurers’ need for rate increases.
The following factors contribute to a large range of average claim by insurer (see Table 9):
Different markets (by affluence; worksite vs. individual; geography; etc.)
Demographic differences (distribution by gender and age)
Distribution by benefit period, benefit increase feature, shared care, and elimination period. For example, one carrier has a higher average home care claim than its average facility claims because home care was a rider and people who added the home care rider were more likely to add compound inflation also.
Distribution by facility-only policies vs. 50 percent home care vs. 100 percent home care vs. home care only.
Different lengths of time in the business.
Differences in the ways insurers report claims.
*The following factors cause our average claim sizes to be understated.
Approximately 16 percent of inception-to-date individual claims are still open and our data does not include reserve estimates for future payments on open claims.
People who recover, then go on claim again, are counted as multiple insureds, rather than adding their various claims together.
Some of our insurers are unable to report how many claimants were paid for care in multiple venues. Because we therefore overstate their number of claimants, we estimate that our overall average claim is understated by roughly $7,000. That is, the average claim has likely been closer to $61,000 than the $54,000 shown in the table above.
Besides being understated, average claim data does not reflect the value of LTCI benefits from some purchasers’ perspectives, because the many small claims drive down the average claim. LTCI provides significant financial yield for most people who need care one year or longer. A primary purpose of insurance is to protect against adverse results, so the amount of protection, as well as average claim, is important.
Six insurers provided their current individual monthly LTCI claim exposure (note: reflects only initial monthly maximum for one insurer). As shown in Table 10, this figure is 29 times their corresponding monthly LTCI premium income and 46.5 times their 2022 LTCI monthly paid claims. Eight insurers contributed data regarding their inforce distribution by benefit period. Treating endless (lifetime benefit periods) as a 15-year benefit period, we found that their average inforce benefit period has reduced to 6.44 years Increasing the assigned value of the endless benefit period by one year has an impact of approximately 0.22 years on the average inforce benefit period. With annual exposure 29 times annual premium and assuming an average benefit period of 6.44 years, we estimate that total exposure is 184 times annual premium. The average benefit period dropped from 7.14 last year to 6.44 this year because one more insurer contributed data and it has by far the lowest average benefit period.
Five insurers reported their current average individual maximum monthly maximum benefit for claimants, with results ranging from $5,393 to $8,309.
Nursing home (NH) claims are more likely to use the policy’s maximum daily/monthly benefit than ALF claims because ALF daily/monthly costs are generally lower and because policies sometimes have lower maximums for ALFs. ALF claims correspondingly are more likely to use the policy maximum than are adult day care and home care claims.
SALES STATISTICAL ANALYSIS Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian, New York Life, Northwestern and Thrivent contributed significant background stand-alone LTCI sales data, but some were unable to contribute some data. LifeSecure provided only total stand-alone sales, not distributions.
Sales characteristics vary significantly among insurers based on market differences (individual vs. worksite, affluence, gender distribution, etc.). Year-to-year variations in policy feature distributions may reflect industry trends but may also reflect changes in participants, participant practices and designs, participant or worksite market shares, etc. In 2021, we had major variance from historical results, and we still have some distortion in 2022 as some participants’ distributions include delayed Washington sales from 2021. Statistical differences between the worksite and non-worksite sales will be reported in the August issue of Broker World.
Market Share We include purchased increases on existing policies as new premium because new coverage is being issued. Table 11 shows 2022 new premium, both including and excluding FPOs. In Table 11, no sales were re-characterized from 2022 to 2021. Total sales levels are remarkably similar to 2020.
Northwestern ranks #1 in new premium both when including FPOs and, for the first time, when excluding FPOs. Mutual of Omaha still ranks #1 in the number of new policies (see Policy Exhibit). Together, Northwestern and Mutual of Omaha account for 65 percent of the market, in terms of premium. When paired with New York Life’s growth, the three top carriers represent 81 percent of the market. The premium below includes 100 percent of recurring premiums plus 10 percent of single premiums.
Worksite Market Share After a high year in 2021 due to the WCF exemption, worksite sales dropped in 2022 as shown in Table 12.
Worksite sales normally consist of three different markets as outlined below, the first two of which produce a higher percentage of new insureds than of new premiums. Worksite 2021 sales were largely voluntary but had the age and premium characteristics of core/buy-up due to Washington sales.
Voluntary group coverage generally is less robust than individual coverage.
Core/Buy-Up programs have particularly young age distributions and modest coverage because a lot of people do not buy-up and are less likely to insure spouses.
Executive carve-out programs generally provide the most robust coverage. One-or two-couple executive carve-out sales may not qualify for a multi-life discount with some insurers, hence may not be labeled as worksite sales in submissions to our survey.
The amount of worksite sales reported and its distribution among the sub-markets significantly impact sales characteristics. Unfortunately, our sales distributions do not reflect the insurers focusing in the group voluntary and core/buy-up markets. More information about worksite sales will appear in the August issue of Broker World magazine.
We noted last year that the future of the non-executive carve-out LTCI market is unpredictable with Transamerica’s departure. Other insurers with stand-alone LTCI products did not absorb Transamerica’s market share. It seems likely that combination worksite products are picking up market share.
Affinity Market Share Affinity groups (non-employers such as associations) produced 5.0 percent of 2022 premium (a relatively low percentage as shown in Table 13) and 7.6 percent of 2022 policies. The percentages in Table 13 reflect only participants’ sales.
Characteristics of Policies Sold Average Premium Per Sale To determine the average premium for new sales, we exclude FPOs. As shown in Table 14, the average premium per new insured and per new buying unit increased substantially over 2020 and prior averages. The key contributor was the reduced percentage of small worksite policies resulting from Transamerica’s departure. Higher prices instituted in late 2020 and early 2021 also contributed to the increase.
The influence of small worksite policies is greatly reduced now. Removing the primary insurer in that market produces an average premium per insured of $3,618, as shown in table 14. Including this carrier produces an average premium of $3,556.
The jurisdiction with the lowest average new premium for participants in 2022 (including FPOs and counting 10 percent of single premiums) was Puerto Rico ($1,270), followed by Alaska ($2,759), which in turn was significantly lower than the third-lowest (Kansas, $3,224). The jurisdiction with the highest average premium was West Virginia ($7,497, a spike caused by two single premium sales; with those removed, West Virginia average would have been $4,952). West Virginia was followed by New England states (which typically have high average premiums)—Connecticut ($5,865), Massachusetts ($5,850), Rhode Island ($5,755), and New Hampshire ($5,611).
Data for 2017 and earlier years included FPOs in these calculations, overstating the average premium per new insured and buying unit.
Issue Age Table 15 shows that 5.8 percent of 2022’s policies were sold to people under age 40, which reflects that delayed Washington sales likely affected our distribution of business when comparing to 2020 levels. The reduction in worksite business does not impact this distribution because starting in 2017, we stopped getting sales distributions from insurers focused on the worksite market.
Last year, we estimated that our participants’ average issue age in Washington was about 15 years lower than outside Washington.
Note: one survey participant has a minimum issue age of 40, one will not issue below 30, and one will not issue below 25.
Benefit Period Table 16 summarizes the distribution of sales by benefit period. The average benefit period rebounded to near 2020 levels but there were still more policies issued with 3-year or shorter benefit periods than any year prior to 2021. Delayed Washington sales likely had some impact here; although, insurers instituted minimum premium rules in Washington in 2021 that likely avoided some short benefit period sales.
Monthly Benefit Monthly determination rebounded to 78 percent of policies sold (Table 17). With monthly determination, low-expense days leave more benefits to cover high-expense days, offering more flexibility for insureds. One insurer offers only daily determination; one insurer offers a choice; and the other insurers automatically have monthly (or weekly) determination.
Despite including some delayed Washington policies, the 2022 sales set the record for the highest average maximum monthly benefit ($5,028) (as shown in Table 18). Sales with an initial monthly maximum less than $3,000 ranged from 2.4 percent of an insurer’s sales to 14.7 percent.
Benefit Increase Features Perhaps because of the reduced amount of worksite business or perhaps because general inflation increased, Table 19 shows that there was an increase in the percentage of policies with 4.5+ percent compounding of benefits. However, despite the general inflation experienced in 2022, protection against future inflation generally decreased, compared to 2020, except for the bounce at 4.5+ percent compounding.
“Indexed Level Premium” policies are priced to have a level premium, but the benefit increase is tied to an index such as the consumer price index (CPI).
As shown in Table 20, we project the age 80 maximum daily benefit by increasing the average initial daily benefit from the average issue age to age 80, according to the distribution of benefit increase features, using current future purchase option (FPO) election rates and a five percent per year offer for fixed FPOs. The maximum benefit at age 80 (in 2045) for our 2022 average 57-year-old purchaser projects to $310/day (equivalent to 2.7 percent compounding). Had our average buyer bought an average 2020 policy two years ago at age 55, her/his age 80 benefit would have been $335/day.
In Table 20, the 2022 figure of $310 might look comparable to the 2020 ($305) and 2019 ($306) figures but note that the 2020 and 2019 projections were to 2042 and 2041, respectively. We project only $4 to $5 more daily benefit to offset inflation to 2045 (3 or 4 more years).
Pandemic protocols are likely to increase facility costs and there are a variety of inflationary pressures which apply to LTC staff salaries at all types of venue. Yet, despite greater awareness of inflation, 2022 purchasers, on average, will have 7.5 percent less coverage at age 80 than would have been the case if they had bought an average 2020 policy in 2020. People are likely to be disappointed by the purchasing power of their policies when they need care if actual cost of care trends exceed the protection built into policies. Policies with flat benefits will experience even greater erosion of purchasing power.
FPOs (Table 21) are important to insureds in order to maintain purchasing power, and 70 percent of our participants’ 2022 FPOs were exercised. The high election rate is noteworthy, considering that the cost increases each year due to larger coverage increases each year, increasing unit prices due to age, and additional price increases due to rate increases.
One participant had an election rate of 96 percent, two had 63 to 68 percent, two had 42 to 51 percent, and one had 12.5 percent. The company with the lowest election rate did not contribute data last year. Participants that reported FPO election rates in both 2021 and 2022 had an increase in election rate from 78.2 percent in 2021 to 88.4 percent in 2022, but the average new premium per FPO election dropped.
Higher election rates occur if FPOs are more frequent (i.e., every year vs. every three years), if elections are “negative-election” (i.e., activate automatically unless the client rejects them) as opposed to “positive-election” (i.e., which activate only if the client makes a request), and if policyholders must exercise FPOs to continue to receive future offers.
FPOs can also be important to insurers. Two insurers got a large percentage of their new premium (42 percent for one; 39 percent for the other) from FPO elections.
Elimination Period Table 22 summarizes the distribution of sales by facility elimination period (EP). The percentage of people buying 84-100 day EP rebounded to more than 91 percent. Two insurers saw 9.6 and 12.2 percent of their buyers choose EPs of longer than 100 days.
Table 23 shows the percentage of participant policies with zero-day home care elimination period (but a longer facility elimination period). The purchase rate of an additional-cost zero-day home care EP option is sensitive to the price. Table 23 shows a drop in 0-day home care EP influenced by Transamerica’s departure from the market.
Table 23 also shows the percentage of participant policies with a calendar-day EP. It is important to understand that most calendar-day EP provisions do not start counting until a paid-service day has occurred. The drop in calendar-day EP results from a change in distribution between carriers.
Sales to Couples and Gender Distribution As shown in Table 24, which summarizes the distribution of sales by gender and partner status, a majority of 2022 purchasers (54.1 percent) were once again female, reversing from 2021.
The percentage of accepted applicants who purchase coverage when their partner is declined dropped below 80 percent for the first time since 2018. It varies significantly by insurer based on their couples pricing and their distribution system. Only two insurers were able to report this data. Their results were similar (77 and 80 percent, respectively) for the percentage of accepted applicants who purchased coverage after a partner’s denial.
Shared Care and Other Couples’ Features Table 25 summarizes sales of Shared Care and other couples’ features.
Shared Care allows one spouse/partner to use the other’s available benefits if their own coverage has been depleted or offers a third independent pool the couple can share.
Survivorship waives a survivor’s premium after the first death if specified conditions are met (such as having been inforce for 10 or more years).
Joint waiver of premium (WP) waives both insureds’ premiums if either insured qualifies for benefits.
Changes in distribution by carrier can greatly impact year-to-year comparisons (Table 25). Some insurers embed survivorship or joint waiver automatically (sometimes only for particular circumstances such as if Shared Care is purchased), while others offer it for an extra premium or do not offer the feature.
In the top half of Table 25, percentages are based on the number of policies sold to couples who both buy (only limited benefit, for Shared Care). The bottom half of Table 25 shows the percentage of policies that results from dividing by sales of insurers that offer the outlined feature. Joint WP and Survivorship had high election rates this year but Shared Care lagged. For insurers reporting Shared Care sales, the percentage of both-buying couples who opted for Shared Care varied from four to 77 percent. The corresponding percentage of couples with Joint WP varied from 10 to 100 percent and for Survivorship ranged from 2.4 to 12.5 percent. Tables 26 and 27 provide additional breakdown on the characteristics of Shared Care sales. Table 26 shows that, for every benefit period except two year, Shared Care was less common than in 2020. The “other” category represents two insurers which reported a few Shared Care sales with benefit periods shorter than two years.
Table 27 looks only at Shared Care policies and reports their distribution across benefit period, so the percentages must total 100 percent. As most policies have three-year benefit periods, most Shared Care policies had a three-year benefit period (Table 27).
Table 26 shows a low percentage of policies having Shared Care, partly because its denominator includes all policies, even those sold to single people or one of a couple. Table 26 denominators are couples who both bought coverage with the particular benefit period. Table 27’s denominator is the number of Shared Care policies.
Shared Care is generally more concentrated in two- to four-year benefit periods than are all sales. Couples are likely to buy shorter benefit periods because couples plan to help provide care to each other and expect the male partner to not need care for a long time. If the female provides care and the male does not need LTC for a long time, more coverage is available for the surviving female when she needs care. As shown in Table 24, single buyers are more likely to be female and females are more likely to opt for a longer benefit period.
Existence and Type of Home Care Coverage Three participants reported sales of facility-only policies, which accounted for 0.3 percent of total sales. One insurer was responsible for 89 percent of such sales. Nearly 96 percent of the comprehensive policies included home care benefits equal to the facility benefit. The other sales all had a home care benefit of at least 50 percent of the nursing home benefit. The last home-care-only sale in our survey was sold in 2018.
Other Characteristics As shown in Table 28, partial cash alternative features (which allowed claimants, in lieu of any other benefit that month, to use between 10 and 40 percent of their benefits for whatever purpose they wish) were included in fewer of our participants’ policies due to a change in market share among participants. One insurer sold 89 percent of such features, which demonstrates how a shift in distribution between insurers can change sales distributions.
Return of premium (ROP) features were included in 7.6 percent of policies. ROP returns some or all premiums (usually reduced by paid LTCI benefits) when a policyholder dies. Roughly 69 percent of ROP features were embedded automatically in the product. Embedded features are designed to raise premiums minimally, typically decreasing the ROP benefit to $0 by age 75. Table 28 shows a large drop in sales with ROP from historical percentages, which reflects not only a change of distribution between insurers but also a change in distribution between products within an insurer. Correspondingly, the percentage of ROP features that were automatically embedded dropped from nearly 90 percent in 2021. The drop is entirely due to one insurer. Collectively, the other insurers had approximately the same percentage as last year.
Restoration of Benefits (ROB), which restores used benefits when the insured has not needed services for, typically at least six months, was included in 17.6 percent of policies with limited benefit periods. Roughly 90 percent of ROB features were automatically embedded.
Insurers must offer shortened benefit period (SBP) coverage, which makes limited future LTCI benefits available to people who stop paying premiums after three or more years. The insurers able to report SBP sales, sold SBP to 4.1 percent of buyers.
Only one insurer issued non-tax-qualified (NTQ) policies, which accounted for 0.1 percent of total industry sales.
“Captive” (dedicated to one insurer) agents produced 58.8 percent of the sales, a large drop from last year’s Washington-driven share (68.6 percent). Brokers produced the balance. Some direct-to-consumer sales were made but not by our participants. At one time, “captive” agents who sold LTCI tended to specialize in LTCI. Now many are agents of mutual companies.
Sales distribution by jurisdiction is posted on the Broker World website.
Limited Pay and Paid-Up Policies In 2022, two insurers in the survey sold policies that become paid-up in 10 years or less, accounting for 1.2 percent of sales.
Because today’s premiums are more stable compared to policies sold years ago, premium increases are less likely. One of the key reasons for buying 10-year-pay (avoidance of rate increases after the 10th year) is greatly reduced, while the cost of 10-year-pay has increased, making it less attractive for consumers than in the past. Nonetheless, limited-pay and single-pay policies are attractive to minimize post-retirement outflow and to accommodate §1035 exchanges. Limited pay sales have been increasing slowly as a percentage of total sales since 2019.
Seven participants reported that 3.6 percent of their inforce policies are paid-up, an increasing percentage as the number of paid-up policies is increasing while the total number of policies is decreasing.
PARTNERSHIP PROGRAM BACKGROUND When someone applies to Medicaid for long-term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (some Indiana and New York policies disregard all assets). Except for California, states with Partnership programs grant reciprocity to Partnership policies issued in other jurisdictions. Partnership programs are approved in 44 jurisdictions, all but AK, DC, HI, MA, MS, UT, and VT. However, MA has a similar program (MassHealth).
Four states (CA, CT, IN and NY) blazed the trail for Partnership programs in the early 1990s. Other states were allowed to adopt simplified and more standardized Partnership regulations as a result of the Deficit Reduction Act of 2005 (DRA).
Approximately 60 percent of Partnership states now allow one percent compounding to qualify for Partnership, which can help low-budget buyers qualify for Partnership and also enable worksite core programs to be Partnership-qualified. A higher percentage of policies will qualify for Partnership in the future if insurers and advisors leverage these opportunities. However, currently only three insurers offer one percent compounding.
Partnership programs could be more successful if:
Advisors offer small maximum monthly benefits more frequently to middle-income individuals. For example, a $1,500 initial maximum monthly benefit covers about four hours of home care every two days and, with compound benefit increases, may maintain buying power. Many middle-income individuals would like LTCI to help them stay at home while not “burning out” family caregivers and could be motivated further by Partnership asset disregard. (This approach does not work in CA, CT, IN and NY because of their high Partnership minimum daily benefit requirements.)
Middle-income prospects were better educated about the importance of benefit increases to maintain LTCI purchasing power and qualify for Partnership asset disregard.
The four original Partnership states migrate to DRA rules.
More jurisdictions adopt Partnership programs.
Programs that privately finance direct mail educational LTCI content from public agencies were adopted more broadly.
Financial advisors were to press reluctant insurers to certify their products and offer one percent compounding.
More financial advisors were certified. Some people argue that certification requirements should be loosened. At a minimum, the renewal certification process could be improved.
Linked benefit products became Partnership-qualified.
PARTNERSHIP PROGRAM SALES Participants reported Partnership sales in 41 states, all authorized states except CA, CT and NY. One carrier sold a Partnership policy in each of the 41 states. One has chosen not to certify Partnership conformance.
Insurance brokers do not have access to Partnership policies in CA, CT and NY and from only one insurer in IN. However, consumers may be able to purchase Partnership-qualified coverage from another entity.
Participants’ Partnership-qualified policies in DRA states rose from 34.6 to 49.9 percent, short of 2020’s 55 percent, presumably influenced by benefit increase provisions being less popular. Minnesota (83.5 percent) leads each year. Wyoming was second (79.5 percent), followed by Maine (73.7 percent) and Wisconsin (70.2 percent). Ten states had between 60 and 70 percent and 23 had at least 50 percent of their policies qualify. Once again, Indiana (5.9 percent) and New Mexico (14.7 percent) were the only states with participant Partnership sales in which fewer than 20 percent qualified.
UNDERWRITING DATA Case Disposition Five insurers contributed application case disposition data to the survey (Table 30). Case resolutions in 2022 were similar to 2020. In 2022, 58.2 percent of applications were placed. One insurer placed 74 percent of its cases; the others placed 50 to 56 percent.
Of cases which were resolved, 28.7 percent were declined or deferred, with the percentage varying from 14.6 to 32.7 percent, depending on insurer. To the degree that a declined applicant got coverage elsewhere or a deferred applicant was ultimately approved, the eventual placement rate for applicants is higher than our data indicates.
Overall, 16.1 percent of cases were suspended or withdrawn during underwriting or not accepted or dropped during the free look period. That is the lowest percentage since 2019. Factors such as age distribution, distribution system, market, underwriting requirements, and underwriting standards affect these results.
Table 31 shows the placement rate by applicant age. This data is a subset of the placement data in Table 30 as some carriers cannot provide this data by age.
Low placement rates increase insurers’ cost per placed policy. More importantly, low placement rates discourage advisors from discussing LTCI with clients. In addition to not wanting to waste time and effort, advisors may fear that declined clients will be dissatisfied. In the Market Perspective section, we listed ways to improve placement rates. This is a critical issue for the industry. If readers have suggestions, they are invited to contact the authors.
Underwriting Tools Five insurers contributed data to Table 32, which divides the number of uses of each underwriting tool by the number of applications processed. For example, the count of instances where medical records were requested was 88 percent of the number of applications. That does not mean that 88 percent of the applications involved medical records, because some applications resulted in more than one set of medical records being requested.
Year-to-year changes in distribution of sales among insurers significantly impact results. Lower maximum ages result in fewer face-to-face exams. Insurers might underreport the use of an underwriting tool because they may lack a good source for that statistic. For example, an insurer might not be able to split phone interviews by whether or not they include cognitive testing.
Underwriting Time Table 33 shows that for six insurers, the average processing time, from receipt of application to mailing the policy, was 49 days. As with other statistics, we believe that our underwriting data overstates the percentage of policies with long underwriting periods because of Washington cases.
Rating Classification Table 34 shows that more than half of 2022 policies were issued in the most favorable rating classification. The table suggests that the percentage of decisions that are either declined or placed in the 3rd or less-attractive classification is reducing slowly, but Table 36 shows that the decline rate was higher in 2022 than in 2020 for each age group. The discrepancy is related to different carriers contributing to the two tables and changing distributions of business.
Tables 35 and 36 show the 2022 percentages of policies issued in the most favorable category and decline decisions by issue age. These tables do not exactly match Table 34 because some participants provide all-age data, rather than separating it by age. The percentage placed in the most favorable classification increased for all ages from 2020 to 2022, at least partly due to changing distribution by age.
The decline rate was higher in 2022 than in 2020 for each age group, even though the younger ages still reflect some 2021 lagged sales. For the past 3 years, the percentage placed in the most favorable classification has been higher for ages 75+ than for ages 70-74 and the decline rate has been lower. The age 75+ block is the smallest and most susceptible to statistical fluctuation, but the primary cause appears to be different distribution of insurers by age. For example, some insurers do not have a “preferred” health discount; the bulk of their policies are issued in their “most favorable” class.
Product Exhibit shows, for 6 insurers: financial ratings, LTCI sales and inforce policies, and product details.
Product Details, a row-by-row definition of the product exhibit entries, with commentary.
Premium Exhibit, which shows lifetime annual premiums for each insurer’s most common underwriting class, for issue ages 40, 50, 60, and 70 for single females, single males, and female/male couples (assuming both are the same age), based on $100 per day (or closest equivalent monthly) benefit, 90-day facility and default home care elimination period (other aspects vary), three-year and five-year benefit periods or $100,000 and $200,000 maximum lifetime buckets, with and without Shared Care and with flat benefits or automatic three and five percent annual compound benefit increases for life. The exhibit includes facility-only policies, as well as comprehensive policies. Worksite products do not reflect any worksite-specific discount.
Premium Adjustments (from our published prices) by underwriting class for each participant.
State-by-state results: percentage of sales by state, average premium by state and percentage of policies qualifying for Partnership by state.
CLOSING We thank insurance company staff for submitting the data and responding to questions promptly. We thank our reader, Ellen Atkins, who suggested we explore the differences in hospice benefits among our participants. We also thank Sophia Fosdick and Quentin Clemens of Milliman for managing the data expertly.
We reviewed data for reasonableness and insurers reviewed their product exhibit displays. Nonetheless, we cannot assure that all data is accurate.
If you have suggestions for improving this survey (including new entrants in the market), please contact one of the authors.
Washington State’s “Washington Cares Fund” (WCF; Revised Code of Washington 50B.04) imposes an uncapped 0.58 percent employee-paid payroll tax ($580 for each $100,000) to fund a $36,500 lifetime pool (intended to inflate, beginning in 2027, according to the Washington consumer price index) for long term care received in WA by vested taxed employees. To qualify, a claimant must require help with at least three activities of daily living. The WCF website lists 11 such activities, one of which is cognitive functioning. In private LTCI, cognitive functioning is a separate trigger, sufficient to justify a LTCI benefit rather than accounting for only one of three required ADL deficiencies.
The bill was signed by Governor Inslee on May 10, 2019, but people who purchased qualifying private stand-alone or combination LTCI by November 1, 2021 could file to be exempt from the tax permanently. As of June 13, 2022,* the state of WA had received 478,173 applications for exemption, approximately 1/8 of the employed population. (*The private LTCI had to be purchased by November 1, 2021, but the exemption request can be filed as late as the end of 2022.)
The repercussions of WCF will be watched closely. When working to get the law passed, proponents expressed confidence that WCF would stimulate a significantly increased future market for private LTCI because WCF would educate consumers regarding their need for LTCI. As WCF is clearly insufficient coverage, consumers would be motivated to supplement WCF coverage. However, the following factors make it questionable that the market will be positively stimulated in the (near) future. (Note: some of these aspects may still be subject to change):
Confusion. Even outside WA, most advisors and consumers consider LTCI to be a confusing product and difficult sale. It is hard for people to remember the triggers and which providers’ services are covered. Selling private LTCI to complement WCF is much more complicated. WCF uses different triggers than the HIPAA-defined triggers used by private LTCI and pays different providers. To the degree that it is hard to remember trigger definitions and provider qualifications, it becomes much more difficult when faced with conflicting definitions.
It is also hard to complement WA-only coverage with national coverage. People who expect to relocate out of WA are more likely to be interested in private LTCI. For them, there is no coverage to complement.
In addition to these major difficulties, there are other complexities. For example, WCF has no daily or monthly maximum nor does it qualify for the state Partnership program.
Dried-Up Stream of Sales. Because Washingtonians wanted to be exempt from the WCF tax, the industry sold more than 90 times as many WA policies with LTCI features in 2021 than in 2020. Because of the avalanche of 2021 sales, demand is likely to be greatly muted for the next several years.
However, a lot of buyers purchased coverage that was less robust than typical previous sales in WA or 2021 sales in other states, so there will be a market to supplement or replace small policies that were purchased. Unhealthy individuals are more likely to want to add to their existing LTCI, likely resulting in a higher decline rate. Such sales require more effort but generate lower-than-average commissions.
Rather than devoting disproportionate attention to WA’s small, unattractive LTCI market, insurers, brokers, employers, and others might sit on the sidelines for an extended period.
Lack of Perceived Need. Many Washingtonians seem likely to think they need no additional coverage. Unfortunately, rather than educate Washingtonians regarding the value of supplemental coverage, the state promotes WCF with messages such as “We no longer have to worry about how we will afford long term care as we age.”
Even those Washingtonians who understand the limitations of WCF coverage may presume the WCF program will be enhanced by the time they might need care, hence not feel motivated to purchase private insurance.
Denigration of the Private LTCI industry. In addition to suggesting that WCF is all the coverage Washingtonians need, WA officials spread inaccurate and misleading comments denigrating private LTCI. If I failed to mention this issue, I would be intentionally suppressing relevant information. I can substantiate this statement, but I don’t want to dwell on this negative point.
Even if WA officials change their tune, a negative impression has been planted in the minds of many current Washingtonians and the inaccurate and misleading information is likely to continue to be quoted and found in internet searches.
Financial advisor hesitance. For several reasons, advisors are reluctant to stray from their areas of expertise. Because of the complications introduced by WCF, financial advisors seem more likely to be hesitant to raise the issue of LTCI with their clients.
The reduced likelihood of a sale also discourages what may be fruitless discussion, and more work for less compensation is not very motivating.
Furthermore, disclosures will be more confusing. Advisors might err or clients might misunderstand or forget what they were told. The resultant increased risk of personal liability for errors or omissions will also discourage some advisors.
Employers and employee benefit managers also seem less likely to be interested. Thus, much of the private LTCI industry might sit on the sidelines for at least several years.
Increased Total Cost. WCF intends to increase benefits, if possible, according to the WA CPI (consumer price index). Historically, the cost of long term care services have increased faster than the CPI. WCF is projected to cover about three months of nursing home care, probably less in some circumstances and over time. The likely shortfall is exacerbated because the CPI factor does not get applied in the first three years of the program and because the initial intended CPI adjustment was delayed 18 months when program implementation was delayed.
As more than 90 percent of LTCI-related policies have a 90-day elimination period (EP), people might conceptually view WCF as covering the elimination period. That’s not accurate, particularly as WCF covers more than 90 days of home care and ALF care. But people want simplifying sound bites. So, the nursing home coverage might cause WCF to be seen as covering the private insurance elimination period.
The combined cost for LTCI (WCF plus private insurance) will increase significantly compared to prior to WCF for two reasons:
Buyers are forced to have a zero-day elimination period which increases the price (but provides additional value).
People who can afford private LTCI tend to be healthy high-earners, who are overcharged for WCF coverage to subsidize less affluent and less healthy Washingtonians.
The market is not likely to respond favorably to the high combined cost. Opting for 180-day EPs is not likely to release the price pressure because the industry traditionally has not lowered prices very much for a 180-day or longer EP compared to a 90-day EP. Longer EPs make insurer results more volatile. A 180-day EP also increases volatility (risk) for the consumer, particularly if they receive long term care services outside WA.
It appears that the WCF is going to be primary coverage, so insurers won’t have to pay benefits for services covered by the WCF. That is appropriate and suggests that insurers might be able to lower premiums. Alas:
To the degree that WCF benefits cover services during the insurer’s EP, there is no cost savings for the insurers. Au contraire, there could be a negative impact because long term care costs are usually lower when the insured bears some of the risk. With a diluted elimination period, the later costs (covered by private LTCI) could be higher.
If claimants are not in Washington, there are no savings.
If claimants are cognitively impaired but don’t satisfy WCF’s criteria, there are no savings. (In private LTCI, cognitive impairment is sufficient to qualify for claims.)
For the above reasons, WCF seems likely to shrink future LTCI sales significantly, particularly stand-alone LTCI sales.
Future sales may migrate heavily toward life insurance or annuities with LTCI features. The life insurance or annuity side of the contract is less confusing and guarantees a pay-out. Because the life/annuity portion predominates, less attention is given to the LTCI elements, which in some cases are incidental additional features. The guaranteed pay-out also causes the buyer to be less concerned about the details regarding LTCI.
A key question relative to the value of LTCI is “How much coverage will insureds have when they need care, which is not likely to occur until they are in their 80s?” The 2021 private LTCI sales in WA were less likely to include automatic compound benefit increases. In addition to providing less coverage up-front, the shortfall is likely to increase over time. Some policies have rights to “future purchase options” (FPOs) to try to maintain the purchasing power of the benefits. I wonder if anyone will compare the future election rate of FPOs on 2021 WA sales to typical industry FPO election rates.
Other Jurisdictions In addition to its impact on future LTCI sales in WA, WCF has encouraged other states to consider state-run LTCI programs. In California, a task force is exploring creation of a state LTCI program. Most observers think a CA-run program is nearly certain. The task force has expressed interest in a program with stronger benefits than WCF. New York (SB 9082), MN (HF 4461) and Pennsylvania (House 2779) have bills. If readers are aware of activity in other jurisdictions, I’d like to be informed.
Before discussing ways in which those programs may differ from WCF, I must poke fun at myself. I told my friends at Milliman that I thought they had overstated the impact of exemptions from the WCF. My argument was that the insurance industry is not very effective in leveraging such opportunities. I was incorrect because I did not appreciate the deluge of demand that WCF created from individuals and employers. I’ve never seen anything like it in my 50 years in the industry. As of June 13, 2022, WA had received 478,173 applications for exemption, which was equivalent to 13.6 percent of WA’s non-farm population. Because people with exemptions are heavily weighted to high earners and young people (who would have paid into the fund many years; or paid fewer years, then left WA without benefits), the cost of the exemptions may exceed Milliman’s estimates.
Other state programs will differ from WCF in terms of exemptions.
To avoid the problem WA experienced, other states will have a much stricter window for exemptions. For example, the NY bill says an individual can qualify for an exemption only if they purchased LTCI prior to January 1 of the year the bill is signed.
The WCF law does not require people to keep their private LTCI in place after they receive their permanent exemption. Other states are likely to close this loophole.
Other states might be more selective as to which policies would qualify for exemption. For example, they might require that the policy qualify for §7702(B). (Washington allowed policies with §101(g) provisions to qualify.) It is less likely, but possible that they might require a compound benefit increase feature.
I expect other states to allow exemptions for people with private LTCI for the following reasons:
It is the right thing to do. Government should encourage citizens to take personal responsibility and reward them for having done so.
By backdating the date that the policy must have been purchased in order to qualify for exemption and by requiring on-going certification, the states avoid giving a tax break to people “gaming” the system.
By allowing exemption, proponents of a state program reduce political opposition to their intended program.
A lot of people who have bought LTCI in the past are retired. It costs nothing to give them an exemption because they wouldn’t be eligible for the program anyway.
Many other people with private LTCI are close to retirement. It might save the state program to allow them to be exempt because they would pay the state LTCI tax for only a few years.
Other jurisdictions may differ from Washington in other respects as well, such as triggers, total coverage, compounding, benefits, vesting, etc.
Hopefully, other jurisdictions will involve the insurance industry in discussions about all aspects of a state-run LTCI program throughout the development process. Such involvement should include front-end salespeople as well as insurance company home office personnel. It should include careful consideration of the insurance industry’s comments, not just token participation.
Increased complexity if multiple states have different programs. Will insurers be interested in complementing state programs if those programs vary by jurisdiction? Will financial advisors consider such complexity worth their effort? Will employers and employee benefit advisors consider LTCI programs if they must vary by employee resident state? What will happen to individuals who move from one state to another? Will inconsistencies increase pressure for a uniform national program? Will consumers, employers, advisors and insurers sit on the sidelines in what they might view as a turbulent market with a questionable future?
Might the history of the state Partnership programs serve as an example? The industry largely spurned the state Partnership programs until DRA 2005 established national standards.
Conclusion: I have no crystal ball to predict the future. Even the WCF itself may change. It will be interesting to see what actually develops.
The 2022 Milliman Long Term Care Insurance Survey, published in the July issue of Broker World magazine, was the 24th consecutive annual review of long-term care insurance (LTCI) published by Broker World magazine. It analyzed product sales, reported sales distributions, and detailed insurer and product characteristics.
From 2006-2009, Broker World magazine published separate group LTCI surveys, but discontinued those surveys when the availability of group LTCI policies shrank. In 2011, Broker World magazine began this August annual analysis of worksite (“WS”) sales to complement the July overall market analysis.
The WS market consists of individual policies and group certificates (“policies” comprises both henceforth) sold with employer support, such as permitting on-site solicitation and/or payroll deduction. If a business owner buys a policy for herself and pays for it through her business, participants likely would not report her policy as a WS policy because it was not part of a WS group. If an employer sponsors general LTC/LTCI educational meetings, with employees pursuing any interest in LTCI off-site, sales would not be reported as WS sales.
We limit our analysis to US sales and exclude “combination” products, except where specifically indicated. (Combination products pay meaningful life insurance, annuity, or disability income benefits in addition to LTCI.)
About the Survey Our survey includes WS sales and statistical distributions from National Guardian Life, New York Life, and Northwestern, and WS sales data from LifeSecure. We estimated sales from four other stand-alone LTCI insurers and compare WS sales to individual LTCI policies that are not WS policies (NWS) and to total sales (Total).
Highlights from This Year’s Survey
As we reported in our July 2022 article, results are heavily influenced by the state of Washington’s “Washington Cares Fund” (WCF, see the “Market Perspective” section for more info). To study the impact of the WCF, we surveyed combination product life insurers in addition to our typical survey of stand-alone LTCI companies. Approximately 60 percent of sales in each line occurred in Washington (“WA”). The industry sold more than 90 times as many stand-alone LTCI policies sales in WA in 2021 than in 2020 and, based on a significant sampling of combination (life and LTCI) policies, that product line also experienced in WA more than 90 times as many sales in 2021 than in 2020.
Driven by WCF’s exemption for private LTCI coverage, we estimate about 9.3 times as many stand-alone WS sales in 2021 (approximately 90,000 in 2021) compared to 2020, while NWS sales increased 47 percent. However, we estimate that new annualized premium grew at a slower pace compared to policy counts—WS premium tripled in 2021 (approximately $60 million in 2021), while NWS premium increased by six percent. The smaller growth in premium arises because the 2021 sales had a higher mix of younger age individuals and a higher mix of less-expensive policies, which was driven by WA sales where individuals sought lower cost policies that would earn exemption from WCF. Our data does not allow us to estimate how much stand-alone LTCI WS sales increased in WA.
Our WS stand-alone statistical distributions can vary significantly from year-to-year because insurers focusing on particular WS markets may be over- or under-represented. We estimate that our statistical distributions reflect only about five percent of WS policies. The carriers providing 2021 statistical data had an average WS annual premium of $2,077 (less than half as much as last year, due to WA sales), whereas the others had an estimated average WS premium of $600, which indicates that our statistical analysis continues to be overly weighted toward executive carve-out programs.
Ten insurers contributed combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual, OneAmerica, PacLife, Securian, and Trustmark. 64.9 percent of their national combined 300,000 sales and 13.4 percent of their national $1.1 billion of new annualized premium were WS sales. Of national WS combined Life/LTCI sales, 73 percent of both the new policies and new premium were in WA. Within WA, 79 percent of new policies and 50 percent of new premium came from WS sales.
Although we have a significant sample, full industry life/LTCI combination sales may differ significantly if our data is over-weighted (or under-weighted) toward WS business, as the WS market grew in WA much more than the NWS market did.
MARKET PERSPECTIVE The three segments of the WS market (which may apply to different employee classes in a single case):
In “core” (also known as “core/buy-up”) programs, employers pay for a small amount of coverage for generally a large number of employees. Employees can buy more coverage. “Core” programs generally have low average ages, short benefit periods, low daily maximum benefits and a small percentage of spouses insured.
In “carve-out” programs, employers pay for robust coverage for key executives and usually their spouses. Generally, executives can buy more coverage for themselves or spouses. Compared to “core” programs, a higher percentage of insureds are married, more spouses buy coverage, the age distribution is older and average premium is higher.
In “voluntary” programs, employers pay none of the cost. The typical coverage is more robust than “core” programs, but less robust than “carve-out” programs. Voluntary programs tend to be most weighted toward female purchasers.
National Guardian, New York Life, and Northwestern write mostly executive carve-out programs and are the only insurers that contributed to our statistical distributions; therefore, our data is heavily-weighted to the executive carve-out market.
Because of tax savings, small executive carve-out issue dates are weighted toward the end of the year. On the other hand, large voluntary cases are traditionally weighted toward fall enrollments with January 1 effective dates. Large voluntary cases are probably more evenly distributed through the year than in the past, but differences remain.
Carrier and product shift: The future of the non-executive carve-out LTCI market is unpredictable with Transamerica’s departure. Even if LifeSecure, Mutual of Omaha, and National Guardian pick up market share, WS stand-alone LTCI sales might drop, at least temporarily because it takes time for competitors to fill in after an insurer drops out.
Particularly for young and less-affluent groups, voluntary programs may gravitate toward products that include life insurance, which is viewed as a more immediate potential need by young employees with families. The possibility of guaranteed issue also draws employee benefit advisors and employers to such products. Such products can allow 100 to 300 percent of the death benefit to be used for LTC, at a typical rate of four percent of the death benefit per month. Unfortunately, combination WS products’ LTCI benefits can lose substantial purchasing power by retirement years because the benefit typically does not increase.
WCF: WA state’s “Washington Cares Fund” imposes a 0.58 percent employee-paid payroll tax to fund a $36,500 lifetime pool (intended to inflate according to the WA consumer price index) for care received in WA as defined in the Revised Code of WA 50B.04. However, people who purchased qualifying private stand-alone or combination LTCI by November 1, 2021 could file to be exempt from the tax. (Note: WCF had received 478,173 applications for exemption as of June 13, 2022.1)
Other jurisdictions may create state-run LTCI programs, but they may not create a window for people to become exempt by buying insurance after the law has passed.
COVID: COVID-19 (COVID) continues to impact the employee benefit market in many ways. As LTCI is generally not perceived to be an urgently-needed benefit, LTCI may be more impacted than some other benefits. Employers potentially have various existential issues that may take precedence over offering LTCI. Staff turn-over is generally higher and more positions are vacant. Shifting of the workforce to remote can be harder to enroll, all else equal.
Nonetheless, COVID did not appear to deter the WA WS sales and, as a result of COVID, there is increased awareness of the LTC risk and of personal exposure and increased interest in staying out of nursing homes. More workers may have elders living in their homes and, if they are remote workers, the needs of those elders are more likely to interfere with their productivity.
Pricing and Underwriting Considerations: Most people interpret Title VII of the 1964 Civil Rights Act to require that employer-involved LTCI programs use unisex pricing if the employer has had at least 15 employees for at least 20 weeks either in the current or previous year. Some states apply similar laws to employers with fewer employees. Thus, for WS sales, insurers must create a separate unisex-priced product. The expense of separate pricing, marketing and administration discourages insurers from serving both the WS and NWS markets.
Moreover, insurers fear anti-selection. Because women have higher expected future claims, unisex pricing saves women money compared to gender-distinct NWS pricing, whereas men pay much more for WS than for NWS policies. The higher the percentage of female buyers in the WS, the more unisex pricing is likely to approach gender-distinct female pricing levels.
Insurers also fear health anti-selection (less-healthy people buying, while healthier people do not buy). Insurers are more vulnerable to health- or gender-anti-selection if the group has a large portion of young or less affluent employees as this group is generally less likely to buy LTCI.
Furthermore, because WS programs rarely offer “preferred health” discounts, healthy couples may pay more for WS coverage than for corresponding NWS coverage. Although there are few health concessions in the stand-alone WS market at this time, some combination products offer guaranteed issue if participation requirements are satisfied.
To control risk, most insurers will not accept a voluntary WS program if there are fewer than 100 employees. However, one insurer (which offers no health concessions) will accept voluntary LTCI programs with as few as 2 to 5 (varies by jurisdiction) employees buying.
In the carve-out market, a more expensive WS product can still produce after-tax savings compared to a cheaper NWS policy, because of tax advantages when an employer pays the premium. The specter of future tax increases enhances the attractiveness of employer-paid premium.
Availability of coverage: Some insurers have raised their minimum issue age to avoid anti-selection (few people buy below age 40) and to reduce exposure to extremely long claims. Such age restrictions can discourage employers from introducing a program, especially a carve-out program if they have executives or spouses under age 40.
With increased remote work, more employers have employees stretched across multiple jurisdictions and eligible non-household relatives might live anywhere. But insurers are less likely than in the past to offer LTCI in jurisdictions with difficult laws, regulations or practices. So, it can be difficult to find an insurer which can cover everyone unless LTCI is sold on a group policy form and the employer does not have individuals in extra-territorial states.
One insurer no longer offers WS LTCI to non-household relatives. Reduced availability for such relatives does not have much impact on sales, because only about one percent of WS sales are to non-household relatives. However, it undermines the suggestion that WS LTCI programs might reduce the negative impact of employees being caregivers.
Prior to gender-distinct pricing, an executive carve-out for two partners of a company with more than 15 employees could have been serviced by any LTCI company, but now it is hard to find a carrier that offers unisex pricing under such circumstances. Such executives may buy policies with gender-distinct pricing either because they are unaware of the requirement under Title VII of 1964 Civil Rights Act; they may disagree with the interpretation that such policies should have unisex pricing to avoid the risk of a civil rights complaint, etc.
Some employee benefit brokers are reluctant to embrace LTCI because of declinations, the effort of enrollment, certification requirements, their personal lack of expertise, etc. WS sales gain from LTCI specialists forming relationships with employee benefit brokers.
Support for Employees who are Caregivers: Various programs offer LTC-related services to employees and their families. Regardless of whether the employee is insured or the relative is insurable, they may be able to access information, advice, services, and products that make caregiving more efficient, more effective, safer, and less expensive. Enabling employees and their families to have better LTC experiences and to use more (not necessarily 100 percent) commercial care should boost productivity at work. Some of these programs are packaged with WS LTCI.
STATISTICAL ANALYSIS As mentioned earlier, insurers’ sales distributions can vary greatly based on the submarket they serve (for example, in the WS market: core, voluntary, or carve-out). Therefore, in addition to fundamental changes in the industry, distributions may vary significantly from year to year due to a change in participating insurers, distribution within an insurer, and market share among insurers. Policies in the carve-out market are designed similarly to those in the NWS market. Our sales distributions reflect only stand-alone LTCI and only about five percent of stand-alone WS policies issued in 2021, unless otherwise noted. The distributions mostly represent the executive carve-out market, as these insurers averaged 10.6 issues per case.
Sales and Market Share Table 1 shows historical WS sales, including some estimates. It shows overall average WS premium for all carriers which reported sales compared to the average WS premium for the participants who contributed statistical data beyond sales. As shown in the table, until 2017, our WS statistics likely represented the broad WS market reasonably. Average premiums plummeted this year because of the WA sales.
Table 2 shows WS sales as a percentage of total LTCI sales, both including estimates. WA sales caused WS sales to be larger percentage of the total compared to past survey data.
Table 3 and the following tables do not include estimates. Thus, Transamerica, which was the #1 insurer in 2020 and 2021, is not included. LifeSecure leapfrogged to the top.
Average Premium Per Buyer Table 4 shows that, in 2021, the average premium per insured in the WS market dropped twice as much from 2020 levels than did the average premium in the NWS market.
As always, the average premium per buying unit (a couple comprise a single buying unit) is higher because there are fewer buying units than insureds. Normally, the increase in average premium per buying unit compared to per insured is significantly lower for WS sales, because more WS buyers are single and because spouses are less likely to buy in the WS. Those factors are muted materially because our data is weighted toward the carveout market. In 2021, the reported differences are small, perhaps influenced by the WA sales.
The average premium per new insured (NB Insured) reflects all participants, but the average premium per buying unit is determined solely by the participants who report sales based on marital status. The WS ratio is probably overstated because participants who reported premium by marital status for the WS are not characteristic of the entire market.
Issue Age In reviewing the balance of the statistical presentations, we urge you to be selective in how you use the data because it is not representative of the entire WS market as explained above.
Table 5 shows that WA sales dropped the average age in the NWS market by 7 years, but only by 3 years in the WS market. If our data included more of the WS market, our WS average age might have dipped more.
Table 7 displays the relative age distribution of workers ages 16+ vs. the age distribution of purchasers in the WS market. It also shows the age distribution of adults 20-79 compared to the age distribution of purchasers in the NWS market. If the percentage of sales in a particular age group is higher than the percentage of population in that age group, the LTCI industry penetrates that age group well. As was the case last year, when we instituted this table, the industry is particularly effective with ages 30-49 in the WS market. In the NWS market, the industry was particularly effective for ages 50-69 last year, but this year broadened the effective range down to 30 because of WA sales.
Rating Classification Most WS sales are in the “best” underwriting class (see Table 8) because there generally is only one underwriting class. Insurers often do not get enough information in WS to determine whether a “preferred health” discount could be granted and use the additional revenue (from not having a “preferred health” discount) to fund extra cost resulting from gender or health anti-selection. Carve-out programs are more likely to offer a “preferred” discount, which means a higher percentage of carve-out policies are issued in the second-best underwriting class. The percentage of policies issued in the best underwriting class soared in the NWS market in 2021 because younger and healthier buyers were drawn to LTCI in WA. The impact on the WS market was smaller, because so few people did not qualify in the best category in 2020. In each market, about 35 percent of buyers who did not qualify for the best price in 2020 shifted into the best category in 2022.
Benefit Period The WS average benefit period is low for core/buy-up programs and somewhat low for voluntary programs. Executive carve-out programs sometimes have longer benefit periods than the NWS market. In 2021, the average benefit period in each market dropped by about a half-year due to WA sales.
The difference in benefit periods between the markets is actually larger than these statistics indicate, because these statistics ignore Shared Care (and the WS market issues much less Shared Care).
Table 10 shows corresponding data back to 2014. As noted elsewhere, this data can jump around based on which insurers provide such detail and whether large core/buy-up cases are written in a particular year.
Maximum Monthly Benefit In 2020, the average initial monthly maximum was about nine percent lower in the WS market than in the NWS market. In 2021, the difference tripled to 27 percent lower in the WS market. To calculate the average initial monthly maximum, we presume an average size in each size range. The $2,100/month we assume for the smallest size range seems to overstate dramatically in 2021 as many people opted for the minimum $1,500/month.
Table 12 shows that the WS initial monthly maximum has varied more over time than the whole market, because of participant changes and how many core/buy-up plans were sold in a particular year.
Benefit Increase Features As shown in Table 13, 95.5 percent of 2021 WS sales had no benefit increase feature or a future purchase option (FPO), hence no first-year premium for benefit increases. The corresponding NWS percentage was 64.1 percent. The corresponding 2020 sales percentages were 86.4 percent and 47.5 percent.
Future Protection Based on a $27/hour cost for non-professional personal care at home ($27 is the median cost according to Genworth’s 2021 Cost of Care Survey), the average WS initial maximum daily benefit of $100 would cover 3.7 hours of such care per day at issue, whereas the typical NWS initial daily maximum of $137 would cover 5.1 hours of such care per day, as shown in Table 14. This year’s higher cost (the hourly cost was $24 in 2020) and lower initial monthly maximums contributed to the 40 percent decrease in WS hours (from 6.2 WS hours) and 25 percent decrease in NWS hours (from 6.8 NWS hours) from last year.
The number of future home care hours that could be covered depends upon when care is needed (we have assumed age 80), the home care cost inflation rate between now (age 39 for WS and 51 for NWS) and age 80 (we have calculated with two, three, four, five and six percent inflation), and the benefit increases provided by the LTCI coverage between now and age 80.
Table 14 shows calculations for three different assumptions relative to benefit increase features:
The first line presumes that no benefit increases occur (either sold without any benefit increase feature or no FPOs were exercised).
The second line reflects the average benefit increase design using the methodology reported in the July article, except it assumes that 40 percent of FPOs are elected (intended to be indicative of “positive” election FPOs, in which the increase occurs only if the client elects it) and provide five percent compounding.
The third line is like the second line except it assumes 90 percent of FPOs are elected (intended to be indicative of “negative” election FPOs, in which the increase occurs unless the client rejects it). It also assumes the FPOs reflect five percent compounding.
Table 14 indicates that:
Without benefit increases, purchasing power deteriorates significantly, particularly for the WS purchaser as younger buyers have more years of future inflation prior to claim onset. With four percent inflation and no benefit increases, the number of covered hours of home care at age 80 dropped from 1.8 for the average 2019 WS buyer to 1.4 for the average 2020 WS buyer, then to 0.7 (only 42 minutes) for the average 2021 WS buyer. For the average NWS buyer, the corresponding hours of home care at age 80 were 3.0 in 2019, 2.9 in 2020, and 1.6 in 2021.
The “composite” (average) benefit increase design assuming that 40 percent of FPO offers are exercised preserves purchasing power better than when no increases are assumed, but still generally leads to significant loss of purchasing power. The average 2021 WS buyer would have 2.1 hours of covered home care at age 80 rather than the 0.7 hours in #1. The average 2021 NWS buyer would have 3.4 hours of covered home care at age 80 rather than the 1.6 hours in #1.
With 90 percent FPO election rates, the average WS and NWS buyers would experience increased purchasing power over time with 3 percent or less inflation but would lose purchasing power with four percent or more inflation.
Table 14 underscores the importance of considering future purchasing power when buying LTCI. Please note:
a) The average 2021 WS buyer was 12 years younger at issue than the average 2021 NWS buyer, hence has 12 more years of inflation and benefit increases in the above table. The actual inflation rate to age 80 is not likely to be the same for today’s 39-year-olds as for today’s 51-year-olds.
b) WS sales have more FPOs, so WS results are more sensitive to FPO election rates.
c) Individual results vary significantly based on issue age, initial maximum monthly benefit, and benefit increase feature, as well as the inflation rate and the age at which the need for care occurs.
d) By the median age of starting to need care (about age 83) and the median age of needing care (about age 85), more purchasing power could be gained or lost.
e) Table 14 does not reflect coverage for professional home care or facility care. According to the aforementioned 2021 Genworth study, the average nursing home private room cost is $297/day, which is currently comparable to 11 hours of non-professional home care. However, the inflation rate for facility costs is likely to differ from the inflation rate for home care. From 2004-2021, Genworth’s studies showed the following compound growth rates: private room in a nursing home (3.0 percent), assisted living facility (3.8 percent), home health aide (2.2 percent), and home care homemaker (2.6 percent).
f) Table 14 could be distorted by simplifications in our calculations. For example, we assumed that the FPO election rate does not vary by age, size of policy or market and that everyone buys a home care benefit equal to the average facility benefit.
g) FPO election rates might be different for policies purchased in 2021. How likely is it that 2021’s WA buyers will exercise FPOs?
Partnership Program Background When someone applies to Medicaid for long-term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (some IN and NY policies disregard all assets). Partnership programs exist in 44 jurisdictions (all but AK, DC, HI, MA, MS, UT, and VT), but MA has a similar program (MassHealth). The first four states to develop Partnerships (CA, CT, IN and NY) have different rules, some of which have become a hindrance to sales. We are not aware of a Partnership-qualified WS LTCI product in those four states, which is unfortunate because the WS market serves many people who could benefit from Partnership.
To qualify for a state Partnership program, a policy must have a sufficiently robust benefit increase feature. Many jurisdictions have lowered the minimum Partnership-eligible compounding benefit inflation rate to one percent. To facilitate Partnership sales in such jurisdictions, an insurer could lower its minimum size by 1/3 (e.g., from $1,500 to $1,000) if one percent compounding is included in a core program. The revenue from the core program would typically increase. The premium would be more level by issue age, shifting risk to the younger ages which can be preferable for the insurer in a core program.
Jurisdictional Distribution Click here for a chart of the market share of each US jurisdiction relative to the total, WS and NWS markets, and the Partnership percentage by state. This chart indicates where relative opportunity may exist to grow LTCI sales.
Elimination Period Approximately 90 percent of the NWS market buys 90-day elimination periods (EPs). For that reason, many WS programs offer only a 90-day EP.
Table 15 shows distribution by EP and how many policies had a 0-day home care feature and a longer facility EP and how many policies had a calendar-day EP (as opposed to a service-day EP). We have reflected that all LifeSecure policies are 90-day EP with a calendar-day definition. Policies which have 0-day home care EP and define their EP as a service-day EP operate almost identically to a calendar-day EP, because people in facilities get daily care.
The large drop in WS 0-day home care EP reflects that Transamerica was in our data last year, but not this year.
Gender Distribution and Sales to Couples and Relatives Insurers began gender-distinct LTCI pricing in 2013, but as explained above, unisex pricing continues in the WS market.
In the NWS market, the 2013-2015 percentages of females were high as insurers that still offered unisex pricing attracted single females. The next 5 years, the percentage of female buyers in the NWS was stable, fluctuating from 54.3 to 54.9 percent. In 2020, women constituted 50.8 percent of the US age 20-79 population2, but in 2021 the percentage of females in the NWS market dipped below 50 percent (49 percent) because of the higher number of males purchasing coverage in WA.
In the WS market, the high percentage of female WS buyers from 2015-2018 suggests that women were particularly attracted to WS LTCI (presumably because of unisex pricing). To the degree that our more recent WS data is over-weighted to executive carve-out programs, it reflects less of the gender anti-selection that likely still exists. Although most executives are male, executive ranks are becoming more gender-balanced and many executive carve-out programs cover spouses. Women make up 47 percent of workers3 but accounted for a bit less (46 percent) of our reported 2021 WS sales. For the third straight year, our data (overly weighted toward executive carveout) has indicated negative gender anti-selection in the WS market, as the 2021 shift to males was stronger in our WS data than in our NWS data.
Table 17 digs deeper, exploring the differences between the WS and NWS markets in single female, couples and Shared Care sales.
Our WS data had fewer single buyers. Despite having more married buyers, there were fewer one-of-a-couple sales and “both buy” couples increased from 45.6 percent of sales to 52.6 percent.
In contrast, the percentage of single people and one-of-a-couple both increased in the NWS market.
Shared Care sales dropped but are likely to rebound in 2021.
Our limited data with regard to relatives who buy shows that two spouses are insured for every three employees. That’s a high percentage reflective of executive carve-out data. Only about one percent of purchasers are relatives other than the employees and employees’ spouses.
Type of Home Care Coverage Table 18 summarizes sales by type of home care coverage. Historically, the WS market sold few policies with a home care maximum equal to the facility maximum. However, with increasing emphasis on home care and simplicity, that difference faded.
Table 18 also shows that monthly determination dominates both markets. The low 2020 monthly determination percentage in the WS was caused primarily by a change in distribution of WS sales among participants.
Many WS products embed a “partial cash alternative” feature (which allow claimants, in lieu of any other benefit that month, to use approximately 1/3 of their benefit for whatever purpose they wish, with the balance extending the benefit period) or a small informal care benefit.
Other Features Table 19 shows that almost all Return of Premium (ROP) features were embedded (automatically included) and phased out before death would be likely. ROP with expiring death benefits may provide an inexpensive way to encourage more young people to buy LTCI but does not address the buyer’s concern (what if I keep paying all my life, then die without qualifying for benefits?).
Table 20 shows lower Joint Waiver of Premium and Survivorship sales to couples in the WS market than in the NWS market, mostly due to differences in distribution by carrier. Some products automatically provide Joint Waiver of Premium if a couple buys identical coverage or if a couple buys Shared Care. Employers sometimes are disinclined to add an optional couples’ feature because they are already contributing more money to cover a married employee plus that employee’s spouse than the cost for a single employee the same age.
CLOSING We thank insurance company staff for submitting the data and responding to questions promptly. We also thank Sophia Fosdick, Rachelle Jacobs, and Zane Truesdell of Milliman for managing the data expertly.
We reviewed data for reasonableness. Nonetheless, we cannot assure that all data is accurate. If you have suggestions for improving this survey, please contact one of the authors.