

The 2024 Milliman Long Term Care Insurance Survey, published in the July/August issue of Broker World magazine, was the 26th consecutive annual review of long-term care insurance (LTCI) published by Broker World magazine. It analyzed product sales, reported sales distributions, and detailed insurer and product characteristics.
From 2006-2009, Broker World magazine published separate group LTCI surveys, but discontinued those surveys when the availability of group LTCI policies shrank. In 2011, Broker World magazine began this annual analysis of worksite (“WS”) sales to complement the overall market analysis.
The WS market consists of individual policies and group certificates (“policies” comprise both henceforth) sold with employer support, such as permitting on-site solicitation and/or payroll deduction. If a business owner buys a policy for herself and pays for it through her business, participants likely would not report her policy as a WS policy because it was not part of a WS group. If an employer sponsors LTC/LTCI educational meetings, with employees pursuing interest in LTCI off-site, sales would likely not be reported as WS sales.
We limit our analysis to US sales and exclude “combination” products, except where specifically indicated. (Combination products pay meaningful life insurance, annuity, or disability income benefits in addition to LTCI.)
The bulk of worksite sales that cover activities of daily living (ADLs) or cognitive impairment do not qualify as LTCI under section 7702(B) and are not covered in this survey (except as specifically mentioned).
In addition to “WS” to represent worksite sales, we use “NWS” to represent individual (non-worksite) sales and “Total” to refer to WS and NWS sales combined.
About the Survey
Participants: Seven insurers (Bankers Life, Knights of Columbus, Mutual of Omaha, National Guardian Life, New York Life, Northwestern, and Thrivent, referred to as “Participants” herein) contribute broadly to stand-alone sales distributions reported herein. Total 2023 sales data includes one additional contributor (LifeSecure) and 2023 inforce data includes two additional contributors (LifeSecure and CalPERS).
Our stand-alone LTCI WS sales and statistical distributions come from participants National Guardian Life, New York Life, and Northwestern; WS sales data from contributor LifeSecure; and inforce business from those insurers plus Mutual of Omaha.
The following ten insurers participated in our combination sales data: AFLAC, John Hancock, Mass Mutual, New York Life, Nationwide, Northwestern Mutual (Northwestern), OneAmerica, Securian, Trustmark and United of Omaha.
Comparisons of sales distributions: WS statistical distributions can vary significantly from year-to-year if particular segments of the WS market are over- or under-represented (the three segments are core, carve-out, and voluntary, described later). Carriers that provided our 2023 distributions had an average worksite annual premium of $2,271, excluding FPOs and single premium policies, whereas insurers that provided sales, but not distributions, had an average annual worksite premium of $1,476. That discrepancy, consistent with the past several years, suggests that our worksite sales distributions are dominated by carve-out executive sales.
Highlights from This Year’s Survey
Table 1 shows WS new sales by year (for 2023: 1,324 lives, down 40 percent from 2022, and $7.1 million of annualized premium, including FPOs, down 18 percent) and Table 2 shows the percentage of Total sales that were made in the WS by year (5.4 percent of lives and 5.9 percent of premium in 2023). The WS stand-alone LTCI market has reduced substantially since the major writer discontinued sales in 2021 and is a decreasing percentage of the Total market. As discussed previously, some sales that are worksite-related may not be classified as WS sales.
Over at least a 20-year period prior to 2022, the fewest stand-alone worksite LTCI policies sold in a year was 8,436 policies (2018). Worksite sales with coverage for ADL-deficiency and cognitive impairment have shifted to combination policies, most of which do not qualify as LTCI under section 7702(B). Only two of the carriers in that market reported combo worksite sales for our survey, but those two carriers sold roughly 80,000 such worksite policies in 2023 (up 16 percent from 2022) compared to the industry’s 1,324 stand-alone LTCI WS sales. Among our combination contributors, WS sales accounted for 36.3 percent of reported lives and 9.9 percent of annualized premium. We have a good-sized sample of combination insurers, but a lower percentage of industry sales than in the stand-alone market.
MARKET PERSPECTIVE
There are three segments of the WS market. A single WS case may involve different segments for different employee classes.
- In “core” (“core/buy-up”) programs, employers pay for a small amount of coverage for generally a large number of employees. Employees can buy more coverage. “Core” programs generally have low average ages, short benefit periods, low daily maximum benefits and a small percentage of spouses insured.
- In “carve-out” programs, employers pay for robust coverage for key executives and usually their spouses. Generally, executives can buy more coverage for themselves or spouses. Compared to “core” programs, a higher percentage of insureds are married and more spouses buy coverage. Because the age distribution is older, the maximum monthly benefit is higher, and the benefit period is longer, the average premium is much higher than for core programs.
- In “voluntary” programs, employers pay none of the cost. The typical coverage is more robust than “core” programs, but less robust than “carve-out” programs. Voluntary programs tend to be most weighted toward female purchasers.
Because of tax savings, small executive carve-out issue dates may have effective dates weighted toward the end of the year. On the other hand, large voluntary cases are more likely to have fall enrollments with January 1 effective dates.
National Guardian, New York Life, and Northwestern write mostly executive carve-out programs and are the only insurers that provided statistical worksite distributions; therefore, our distributions are heavily weighted to the executive carve-out market.
Carrier and product shift: Voluntary WS programs have gravitated toward combination products that include life insurance because insurers, brokers, employers, and employees tend to favor combination products.
Insurers’ pricing, underwriting, and distribution considerations favor combination products. Prior to 2012, insurers used unisex “street” pricing and typically discounted “street” prices by five percent for the worksite. Gender-distinct “street” pricing made WS pricing more complicated for insurers who believe unisex pricing is preferable in the WS due to Title VII of the 1964 Civil Rights Act. Pricing, state filing, administration, and illustration work increased when insurers could no longer simply reduce “street” prices by five percent.
Because women have higher expected future claims, unisex pricing saves women money compared to gender-distinct NWS pricing. On the other hand, men pay much more (e.g., roughly 50 percent more for some insurers) with unisex pricing than with gender-distinct pricing, possibly complicating WS sales and raising insurer concerns about gender anti-selection (a higher percentage of females in WS cases).
Insurers also fear health anti-selection (unhealthy people being over-represented among buyers), as stand-alone LTCI does not have a high voluntary participation rate. Therefore, WS stand-alone LTCI programs have limited, if any, underwriting (health) concessions.
Combination products with LTC-related benefits are less affected by unisex pricing as females pay less for the death benefit but more for the LTCI (or chronic illness) benefit. Furthermore, products with chronic illness riders do not require salespeople to be LTCI-certified, which provides insurers access to a broader distribution system than with stand-alone LTCI. As combination life programs have higher penetration rates, insurers often offer “guaranteed issue,” coverage based on the number of employees and participation rates.
From the broker, employer, and employee perspective, simplicity is very attractive. “Guaranteed issue,” along with typically fewer age restrictions than for unisex stand-alone LTCI pricing, allows any employee to be covered and makes enrollment easier and faster, like other employee benefit offerings.
Additionally, combination products’ death benefit avoids the “use it or lose it” issue and is more meaningful for young and less affluent people than is LTCI. Such products can allow 100 to 300 percent of the death benefit to be used for help with ADLs or cognitive impairment, typically using up to four percent of the death benefit each month. Alternatively, they can allow 100 to 200 percent of the death benefit (at a rate of four percent per month) but restore the death benefit each month when a LTCI claim is processed. With “restoration”, beneficiaries will receive the full death benefit regardless of how much LTCI benefit was received. Most of these provisions qualify as “chronic illness” under IRS §101(g); others qualify as “long-term care insurance” under IRS §7702(B). The chronic illness products do not require broker LTCI certification, which makes those products “simpler” than §7702(B) products.
While stand-alone (and linked-benefit) individual LTCI products generally offer annually-increasing coverage to try to maintain purchasing power in the face of inflationary increases in the costs to provide long-term care, WS combination products have a fixed benefit. For example, if a 30-year-old employee buys a $100,000 death benefit, she will have a $4,000 monthly benefit for chronic illness (assuming the benefit features described above). That $4,000 benefit would have much more purchasing power if she needs care in the next few years than if she needs care 50 years from now.
Stand-alone LTCI is still popular in executive carve-out programs. Executives can more easily afford to continue coverage after termination of employment, hence appreciate the value of compound benefit increases. Income tax advantages encourage employer-paid coverage, particularly for executives, and tax advantages may increase in the future if income tax rates rise or if such LTCI coverage permits opting out of future state LTCI programs. Because of tax advantages and employer premium payment, higher unisex prices for men are less of an issue in the executive carve-out market. Two stand-alone LTCI insurers offer unisex pricing with as few as 2 to 5 (varies by jurisdiction) employees buying, an approach that caters to this market.
State-run LTCI programs: We discussed state-run LTCI programs in the July/August issue and prior years’ articles. Washington state’s “Washington Cares Fund” (WCF) stimulated tremendous market demand in the state of Washington, causing WS sales and distributions to vary greatly from historical trends in 2021 and 2022. However, the Washington Cares Fund and other potential state-run programs appear to have had little impact on 2023 WS sales.
Availability of coverage: As few people younger than age 40 buy stand-alone LTCI, some insurers have raised their minimum issue age to avoid anti-selection and to reduce exposure to extremely long claims. One insurer limits the maximum age to 69. Such age restrictions can discourage employers from introducing a program (even a carve-out program if they have executives or spouses too young to be covered).
Younger employees who are ineligible for coverage may still benefit from a program because their elders are often eligible for WS stand-alone LTCI programs. However, one contributor no longer offers WS LTCI to non-household relatives. Reduced availability for such relatives does not have much impact on sales, because typically 99 percent of worksite sales are to employees or their partners. Thus, even if a program is available to elder relatives, it is not likely to meaningfully address the negative impact of employees being caregivers.
With increased remote work, more employers have employees stretched across multiple jurisdictions. Eligible non-household relatives might live anywhere. However, insurers may not offer a product in jurisdictions with difficult laws, regulations, or practices, such as slow policy form approval. It can be hard to find a product which can cover everyone unless LTCI is sold on a group policy form and the employer does not have individuals in extra-territorial states. Combination products also run into jurisdictional issues because some jurisdictions do not allow LTCI benefits to exceed the death benefit and/or do not allow death benefit restoration.
Increasing hurdles for coverage have discouraged brokers as well as insurers. Some employee benefit brokers are reluctant to embrace stand-alone LTCI because of declinations, the enrollment effort compared to typical group coverages, certification requirements, their personal lack of expertise, etc. These issues could be mitigated by LTCI specialists forming relationships with employee benefit brokers.
Support for Employees who are Caregivers: Various programs offer LTC-related services to employees and their families. Regardless of whether the employee is insured or the relative is insurable, they may be able to access information, advice, services, and products that make caregiving more efficient, more effective, safer, and less expensive. Enabling employees and their families to have better LTC experiences and to use more (not necessarily 100 percent) commercial care should boost productivity at work. Some of these programs are packaged with WS LTCI.
STATISTICAL ANALYSIS
In addition to fundamental industry changes, distributions may vary significantly from year to year due to different participants, shifting distribution within an insurer, and changing market share among insurers. Our sales distributions reflect only stand-alone LTCI. Two insurers reported their number of new employer cases as well as the number of new worksite sales. Combined, they averaged 5 applications per new employer case, which seems to confirm the executive carve-out concentration in our data.
Aggregate Sales
Table 1 shows the number of sales and premium in the worksite market by year. As noted above, the worksite market is in decline, with the exception of 2021 due to sales stimulated by the WCF. The shrinkage of the stand-alone WS market is underscored when you consider that nearly two-thirds of 2023 WS premiums came from FPOs on past years’ sales.
Table 2 shows WS sales as a percentage of total LTCI sales. As the market shrinks, the impact of FPOs on past sales becomes larger. FPOs account for WS being a higher percentage of premium (5.9 percent) than policies (5.4 percent). Removing FPOs, the WS premium is 3.2 percent of the total. The 2022 percentages are slightly inflated due to runout sales in Washington.
Market Share
Table 3 shows the insurers’ reported WS sales, including FPOs and new sales to worksite cases issued in prior years. Excluding FPOs, New York Life would have been in the lead, followed by LifeSecure.
Average Premium Per Buyer
Table 4 shows the average premium (without FPOs and without single premiums) per new insured for WS contributors, for WS participants (insurers which provided distributions), and for the NWS market. The total WS market has a lower average premium than those WS carriers that provided distributions. When comparing the WS market to the NWS market, influences such a younger average issue age drive the lower WS average premium.
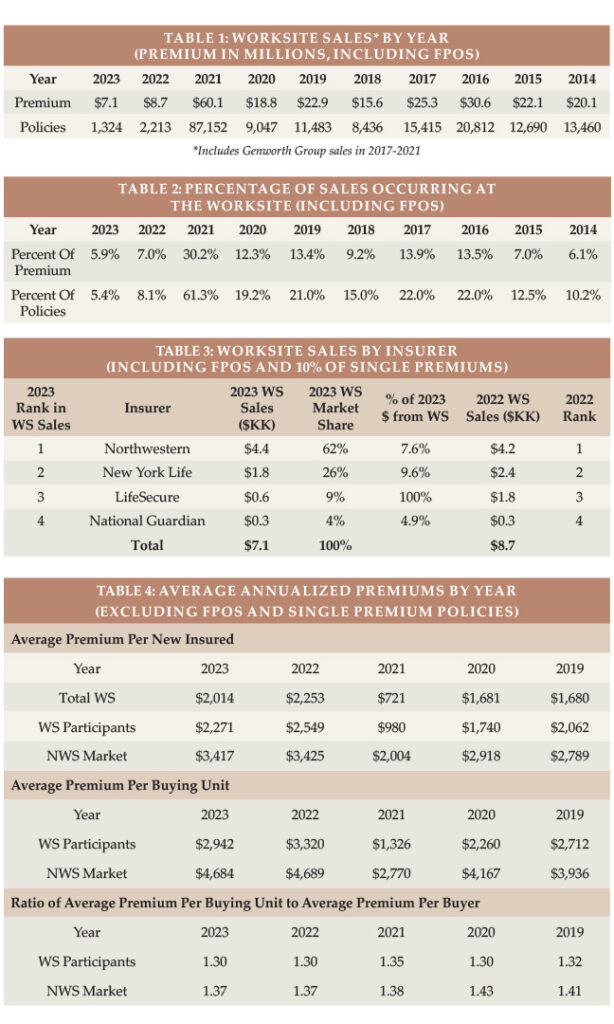
Table 4 also shows the average premium per buying unit for insurers that provided distributions (a couple comprise a single buying unit). The average premium per buying unit is higher because there are fewer buying units than insureds. The ratio between average premium per buying unit and average premium per insured life is consistently lower for WS sales, because more WS buyers are single and because spouses are less likely to buy in the WS. However, Table 4 likely understates the difference because our WS distributions reflect a higher concentration from the carveout market, which has a lot of couples who both buy.
Issue Age
In reviewing the balance of the statistical presentations, we urge you to be selective in how you use the data because it is not representative of the entire WS market as explained above.
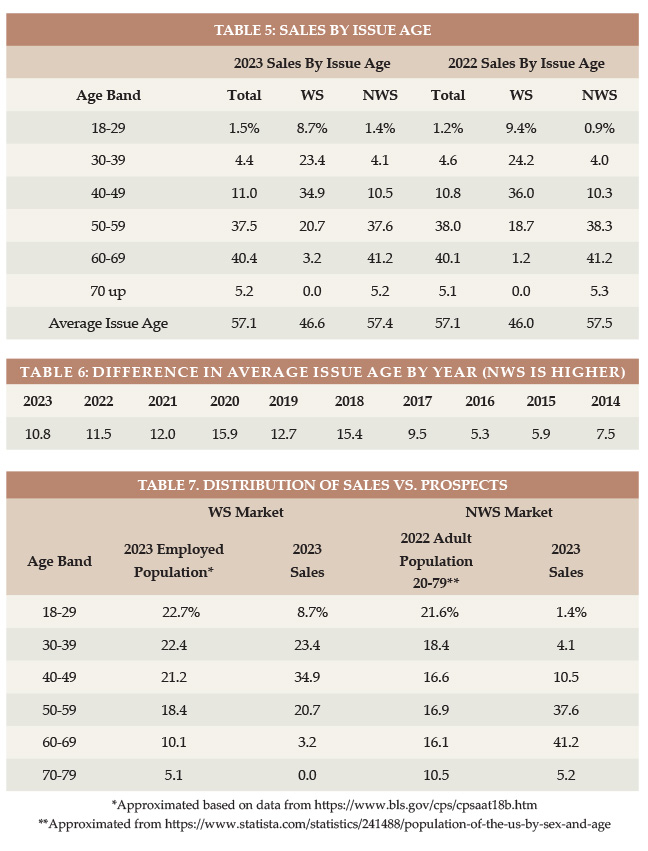
Table 5 shows the distributions by issue age and Table 6 shows, by year, how much older the average age NWS buyer is than the average age WS buyer.
Table 7 displays the relative age distribution of workers ages 18+ compared to the age distribution of purchasers in the WS market and the age distribution of adults 20-79 compared to the age distribution of purchasers in the NWS market. If the percentage of sales in a particular age group is higher than the percentage of population in that age group, we can conclude that LTCI is more appealing to that age group, the industry gets in front of that age group more, and/or more of the applicants in that age group qualify for coverage. In the WS market, the industry is particularly effective with ages 40-49. In the NWS market, the industry is particularly effective for ages 50-69.
Rating Classification
Three of our seven contributors do not offer a “preferred health” discount, so the bulk of their sales are in their best underwriting class. They are also the insurers providing WS distributions, which contributes to the high percentage (92 percent) of worksite policies issued in the best underwriting class, as shown in Table 8.

Benefit Period
The WS average benefit period is low for core/buy-up programs and somewhat low for voluntary programs. Executive carve-out programs sometimes have longer benefit periods than the NWS market. In 2023, the WS market, for the first time since 2016, had a slightly longer average benefit period than the total market (see Table 9). Table 10 shows the results by year. Note that these statistics ignore Shared Care which, in effect, lengthens benefit period and is more prevalent in the NWS market.
Maximum Monthly Benefit
To calculate the average initial monthly maximum, we presume an average size in each size range shown in Table 11. While the WS market had a slightly longer average benefit period in 2023 than did the NWS market, it had a smaller average initial monthly maximum.
Table 12 shows that the initial maximum monthly benefit hit record high levels in 2023. The WS initial monthly maximum varies more over time than the total market because of participant changes and how many core/buy-up plans were sold in a particular year.

Benefit Increase Features
As shown in Table 14, 10.8 percent of 2023 WS sales had compounding of three percent or higher, compared to 9.1 percent in 2022. Of the 2023 WS sales, 17.4 percent had no increase feature and 67 percent had a FPO feature.
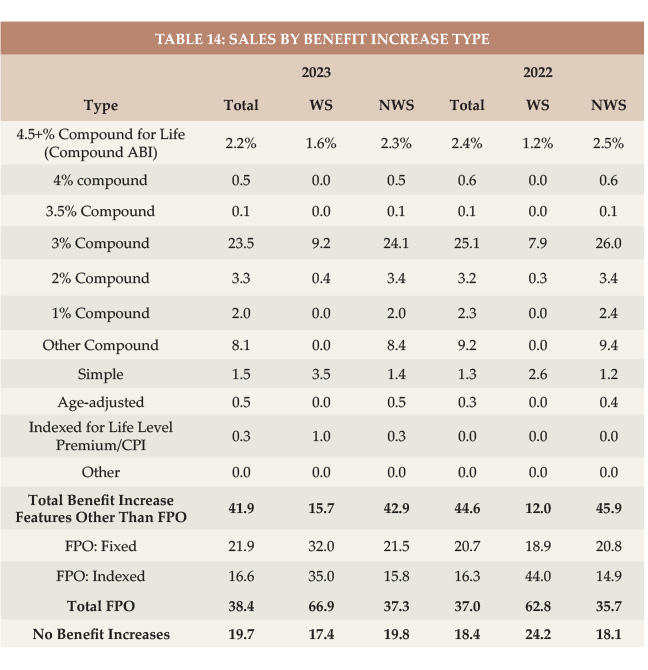
In the NWS market, 26.9 percent had three percent or higher compounding compared to 29.2 percent in 2022. While three percent or more compounding is dropping in the NWS, it is increasing in the WS market, albeit still much less common in the WS market.
Future Protection
Based on a $33/hour cost for home health aides (the median cost according to Genworth’s 2023 Cost of Care Survey), the average WS initial maximum daily benefit of $166 would cover 5.0 hours of such care per day at issue, whereas the typical NWS initial daily maximum of $173 would cover 5.2 hours of such care per day, as shown in Table 15.
The number of future home care hours that could be covered depends upon when care is needed (we have assumed age 80), the home care cost inflation rate between now (age 47 for WS and 57 for NWS) and age 80 (we have calculated with 2, 3, 4, 5 and 6 percent inflation), and the benefit increases provided by the LTCI coverage between now and age 80.
Table 15 shows calculations for three different assumptions relative to benefit increase features:
- The first line presumes that no benefit increases occur (either sold
- without any benefit increase feature or no FPOs were exercised).
- The second line reflects the average benefit increase design using the methodology reported in the July/August article, except it assumes that 40 percent of FPOs are elected (intended to be indicative of “positive” election FPOs, in which the increase occurs only if the client elects it) and provide five percent compounding.
- The third line is like the second line except it assumes 90 percent of FPOs are elected (intended to be indicative of “negative” election FPOs, in which the increase occurs unless the client rejects it). It also assumes the FPOs reflect five percent compounding.
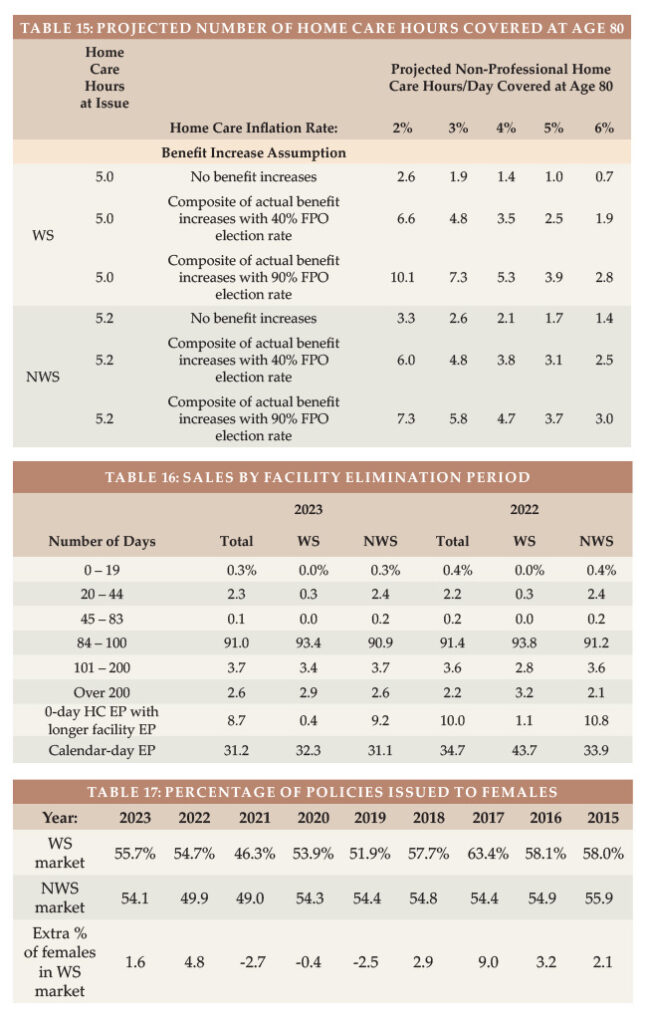
Table 15 indicates that:
- Without benefit increases, purchasing power deteriorates significantly, particularly for the WS purchaser as younger buyers have more years of future inflation prior to claim onset. For example, with a flat benefit, the number of covered hours of home care at age 80 drops to 1.9 hours for the average WS purchase age if there is three percent inflation. The average NWS buyer would have 2.6 hours of care (rather than 1.9 hours) at age 80 if they had no benefit increases and inflation was three percent because the average NWS buyer is older (and secondarily, buys a larger daily benefit).
- The “composite” (average) benefit increase design assuming that 40 percent of FPO offers are exercised preserves purchasing power better than when no increases are assumed. The average WS buyer gains buying power over time if the inflation rate is two percent, being able to pay for 6.6 hours at age 80. But if the inflation rate is four percent, this drops to 3.5. The average NWS buyer generally does better because of a higher issue age, more robust benefit increase features and a higher initial maximum daily benefit. However, the WS market has more FPOs, so when we assume 90 percent FPOs election, the WS market does better. It also does better with 40 percent FPO election and a two percent inflation rate because we presume a full five percent FPO will be exercised.
Assuming that 90 percent of FPO offers are exercised, the average WS buyer would have at least as much coverage at age 80 as at issue if the inflation rate is less than four percent. The average NWS buyer has increasing purchasing power unless inflation averages four percent.
Table 15 underscores the importance of considering future purchasing power when buying LTCI. Please note:
a) The average 2023 WS buyer was 10 years younger at issue than the average 2023 NWS buyer, hence has 10 more years of inflation and benefit increases in Table 15. The actual inflation rate to age 80 is not likely to be the same for today’s 47-year-olds as for today’s 57-year-olds.
b) Individual results vary significantly based on issue age, initial maximum monthly benefit, and benefit increase
feature, as well as the inflation rate and the age at which the need for care occurs.
c) By the median age of starting to need care (about age 83) and the median age of needing care (about age 85), more purchasing power could be gained or lost.
d) Table 15 does not reflect coverage for professional home care or facility care. According to the 2023 Genworth study, the median nursing home private room cost is $320/day, which is currently comparable to 10 hours of non-professional home care. However, the inflation rate for facility costs is likely to differ from the inflation rate for home care. From 2004-2023, Genworth’s studies showed the following compound growth rates: private room in a nursing home (3.1 percent), assisted living facility (4.3 percent), home health aide (2.7 percent), and home care homemaker (3.1 percent).
e) Table 15 could be distorted by simplifications in our calculations. For example, we assumed that the FPO election rate does not vary by age, size of policy or market and that everyone buys a home care benefit equal to the average facility benefit.
Partnership Program Background
When someone applies to Medicaid for long-term care services, most states with Partnership programs disregard assets up to the amount of benefits received from a Partnership-qualified policy (with some policies, IN and NY disregard all assets). Partnership programs exist in 44 jurisdictions (all but AK, DC, HI, MA, MS, UT, and VT), but MA has a similar program (MassHealth). The first four states to develop Partnerships (CA, CT, IN and NY) have different rules, some of which have become a hindrance to sales. We are not aware of a Partnership-qualified WS LTCI product in those four states, which is unfortunate because the WS market serves many people who could benefit from Partnership.
To qualify for a state Partnership program, a policy must have a sufficiently robust benefit increase feature. At least 29 jurisdictions have lowered the minimum Partnership-eligible compounding benefit inflation rate to one percent. To facilitate Partnership sales in such jurisdictions, an insurer could lower its minimum size from $1,500 to $1,000 if one percent compounding is included in a core program. The policies would qualify for the state Partnership and case revenue and core sales would likely increase. The premium would be more level by issue age, shifting risk to younger ages which can be preferable for the insurer in a core program.
Jurisdictional Distribution
We also examined the market share (based on number of new insureds) by jurisdiction. As was the case last year, the WS market share of five states (AL, AK, HI, NC, & VT) was at least 50 percent higher than that state’s overall market share (e.g., if they had a two percent overall market share, they had at least a three percent market share in WS). This could be the result of a single large case in that state. In 18 jurisdictions (same number as last year), the market share of total sales was at least 50 percent greater than the WS market share, suggesting that there may be opportunity for WS sales in these jurisdictions: CO, DE, IN, KS, KY, LA, MA, MD, ME, MO, MS, NE, NH, NV, OR, RI, SD, and VA. (The 9 bold italicized states were in this list last year.) In 7 jurisdictions (up from 5), our participants had no stand-alone WS sales at all (DC, ID, NM, UT, WV, WY and Puerto Rico).
Click here for a chart of the market share of each US jurisdiction relative to the total, WS and NWS markets, and the Partnership percentage by state. This chart indicates where relative opportunity may exist to grow LTCI sales.
Elimination Period
More than 90 percent of the NWS market buys 90-day elimination periods (EPs). For that reason, many WS programs offer only a 90-day EP.
Table 16 shows distribution by EP and how many policies had a 0-day home care feature and a longer facility EP and how many policies had a calendar-day EP (as opposed to a service-day EP). We have reflected that all LifeSecure policies are 90-day EP with a calendar-day definition. Policies which have 0-day home care EP and define their EP as a service-day EP operate almost identically to a calendar-day EP, because people in facilities get daily care.
Gender Distribution and Sales to Couples and Relatives
Insurers began gender-distinct LTCI pricing in 2013, but unisex pricing continues to be typical in the WS market because of Title VII of the 1964 Civil Rights Act.
Women are 49.9 percent of the US age 20-79 population but have nearly always dominated LTCI sales1. Since 2016, the percentage of female buyers in the NWS has fluctuated from 54.1 to 54.9 percent (see Table 17), except for 2021 when the percentage of females dipped below 50 percent in both the WS and NWS markets because of the higher number of males purchasing coverage in WA. In 2022, the NWS market also had fewer than 50 percent females because of delayed processing of 2021 WA sales, but the Total market reverted to mostly female.
Table 17 also shows that the WS market generally experiences a higher percentage of female buyers (presumably because of unisex pricing), quantifying the above-mentioned “gender anti-selection” compared to the NWS market. To the degree that our WS data is over-weighted to executive carve-out programs, it likely understates the gender anti-selection of voluntary WS LTCI programs. Women make up 46.9 percent of workers but accounted for 55.7 percent of our reported 2023 WS sales2.
Table 18 digs deeper, exploring the differences between the WS and NWS markets in single female, couples, and Shared Care sales.
Our WS data has more couples who insure only one partner (59.6 to 49.8 percent in the NWS market). Shared Care is less often offered in a WS program.
Our limited data with regard to relatives who buy shows that two spouses are insured for every three employees. That’s a high percentage reflective of executive carve-out data. Over time, we have seen about one percent of purchasers are relatives other than the employees and employees’ spouses.
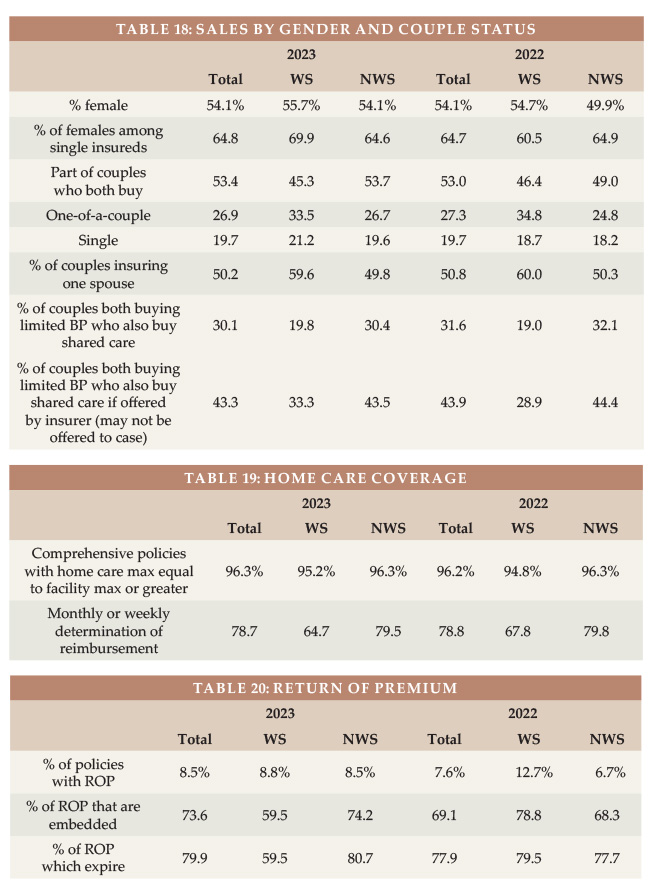
Type of Home Care Coverage
Table 19 summarizes sales by type of home care coverage and shows the frequency of monthly determination of benefits. Long ago, WS policies’ home care maximum monthly benefits were 50 percent of the facility benefit; today they are generally identical.
Other Features
Table 20 shows that most Return of Premium (ROP) features are automatically included and phase out before death would be likely. ROP with expiring death benefits may provide an inexpensive way to encourage more young people to buy LTCI but does not address the buyer’s concern that they might pay all their life, then die in their 90s without qualifying for benefits.
Table 21 shows lower Joint Waiver of Premium and Survivorship sales to couples in the WS market than in the NWS market. Some products automatically provide Joint Waiver of Premium if a couple buys identical coverage or if a couple buys Shared Care. Employers sometimes are disinclined to add an optional couples’ feature because they are already contributing more money to cover both a married employee and that employee’s spouse than the cost for a single employee the same age.
CLOSING
We thank insurance company staff for submitting the data and responding to questions promptly. We also thank Sophia Fosdick and Quentin Clemens of Milliman for managing the data expertly.
We reviewed data for reasonableness. Nonetheless, we cannot assure that all data is accurate. If you have suggestions for improving this survey, please contact one of the authors.
References
1. https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age/
2. Bureau of Labor Statistics, https://www.bls.gov/cps/cpsaat18b.htm




