Actionable Intelligence in Long-Term Care Planning
When Oliver Wyman and Ice Floe Consulting embarked on our agent and advisor survey, called Who is Selling What? To Whom? How & Why? (WWWHW), we wanted to explore the salesperson’s view of:
- Best practices in starting the long term care planning conversation.
- Agent/advisor/consumer product perceptions and preferences.
- Best ways to get prospects and clients to “yes.”
- New product insights.
- Types of training and education that will improve sales results.
- Why many agents/advisors do not discuss long term care planning with consumers.
There is more to building a survey like this than meets the eye. Some of the issues we grappled with included:
- Determining our audience; we needed to approach a large and varied swath of insurance agents, financial advisors and legal and accounting professionals who would share their views.
- Identifying topics and crafting questions that would provide meaningful responses and actionable intelligence.
- Deciding to “go long or short.” Surveys that want big numbers of responses are generally short. However, we wanted to get a complete picture of the topics involved. Therefore, we chose to “go long.”
To accomplish these goals, we contacted hundreds of thousands of licensed agents and financial advisors through various channels. With the help of Broker World Magazine, NAIFA, NAILBA, Center for Long-Term Care Reform, and independent life and long-term care insurance distribution, we “pounded the airways” with email outreach. Additionally, we purchased a list of 400,000 licensed life and health agents to ensure we had a representative sample.
As a result, we received tens of thousands of answers from over 600 agents/advisors who completed all or part of the survey. As of this writing, we are still analyzing responses and cross-referencing related questions to identify key takeaways. However, we can now share a high-level view of some data we have obtained.
Who is Selling?
There is a committed and well-trained group of agents/advisors that do take long term care planning seriously. While they may consider themselves “specialists,” do not confuse this term with “exclusivity.” The majority of survey respondents consider long term care planning part of a broader insurance or financial services practice, which may include life, health, Medicare, property/casualty, tax planning, legal, estate and business insurance, and employee benefits. These agents/advisors work with various distribution channels, with the majority in the “independent” category. Most respondents have been an agent or financial advisor for more than 16 years and are 51 years or older, with most being over 60. Interestingly, a significant number of survey respondents indicated they refer clients to a long term care planning specialist as opposed to handling it themselves.
Our initial takeaways from this high-level data are:
- Interest in long term care planning cuts across many different areas of practice.
- Numerous agents/advisors are aging out of the business.
- Interest in including long term care planning in agent/advisor practice is wide but not deep.
- Insurance companies and distributors have a major opportunity to focus younger agents/advisors on long term care planning.
- Younger agents/advisors should consider this a “Blue Ocean” opening to expand their business practice.
What?
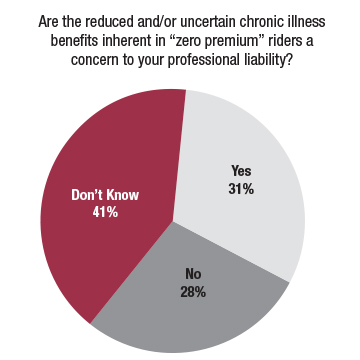
Let us start with a point of context. The sale of life insurance policies with long term care or chronic illness benefits have grown significantly over the past five years. It is important to note, however, that in 2019, 59 percent of all combo products sold included “zero-premium living benefit” riders.1 Life policies that utilize this form of chronic illness benefit provide indeterminate long term care planning value that isn’t generally apparent until time of claim. A majority of respondents expressed concerns over the professional liability issues inherent in selling “long term care planning solutions” without benefits that were clearly delineated. Additionally, they struggle with trying to explain “discounted” and “lien” methods of chronic illness benefit payment.
Our agent/advisor survey respondents clearly indicated a preference towards traditional stand-alone long term care insurance and combo plans that included long term care accelerated death benefits and/or extension of benefit riders. It does not appear that chronic illness accelerated death benefit riders with contractual language and benefit payment methods similar to long term care riders appeal to many agents/advisors. It is not clear from the LIMRA data which insurance companies are using updated best practices re the HIPAA claims qualifying definition. We believe this contractual language matters to agents/advisors and consumers. Agents/advisors also indicated the expansion of life combo policies offering recurring premium options have made these products more accessible to more consumers.
Our initial takeaways from this data are:
- Utility and value of “zero-premium living benefit” riders are unclear to agents/advisors or consumers.
- Agents/advisors prefer long term care benefits over chronic illness benefits.
- Entry-level premium matters.
Who is the Customer?
Agents/advisors agree that the best client to have a long term care planning discussion with has had a family member who needed long term care and/or they have been a caregiver themselves. Cost of care, desire not to be dependent on family, and control over type and location of long term care services are key consumer motivators.
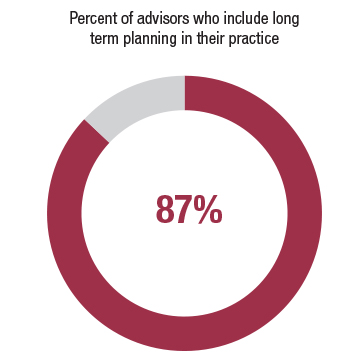
Considering that most of our respondents actively include long term care planning in their insurance and financial practices, it comes as no surprise that they proactively have the conversation with clients and have a high comfort level doing so. However, this comfort level may be exaggerated by our survey sample. A 2017 Consumer/Advisor survey by Lincoln Financial Group found that 28 percent of advisors found it difficult to discuss long term care with their clients, while only 12 percent of our respondents found it so. The Lincoln Financial Group2 survey reported that 76 percent of consumers would find it valuable if their advisor discussed long term care planning with them. Coincidentally, our survey respondents indicated that 75 percent of the time they raise the planning idea before their clients do.
Our initial takeaways from this data are:
- Experiencing the hard truths of the long term care event continues to be a primary consumer motivator.
- Proactive and systematic inclusion of the long term care planning discussion leads to sales success.
- If the agent/advisor waits to be ”asked,” they either missed the sales opportunity or it is probably too late to help.
How–Best Practices–Is the Sale Made?
“Nothing happens until a sale is made.” These immortal words by Thomas J. Watson, Sr., speak directly to the proactive nature of sales success. With this in mind, we wished to determine if there are unifying practices successful agents/advisors use as they navigate consumers through the long term care planning discussion. Approximately 40 percent of those surveyed indicated the conversation began as a specific “dominant need” conversation. An almost equal number said long term care planning was part of their overall financial design process. Sixteen percent said the discussion was part of their life insurance review activity.
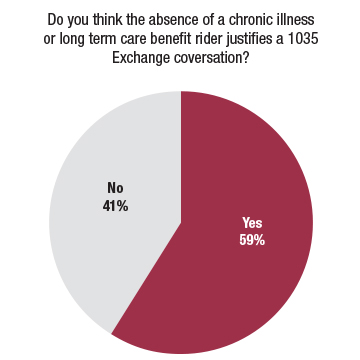
“Upgrading” an existing life insurance policy to include long term care or chronic illness benefits was a key talking point for agents/advisors. 1035 Exchange opportunities also came into play when appropriate. The top three client “screening” techniques continue to be health evaluation and insurability assessment, financial appraisal, and discussion of personal financial goals. Ultimately, however, the sale continues to be fueled by experience with long term caregiving.
Why?
As we have said in the corporate boardrooms of insurance companies, prior to a consumer purchasing a life or long term care insurance policy an agent/advisor must believe that risk is real and the product they are offering has value. It is clear from our survey that the respondents are passionate about long term care planning. Many own it themselves, have had long term caregiving experiences and believe it is the cornerstone of a complete financial plan. From our experience these are universal traits of most successful life/long term care insurance professionals. The big questions for insurance companies and distribution is: How do we imbue more producers with these attitudes and enthusiasm?
Takeaways for Another Day
As we analyze and correlate survey responses with the team at Oliver Wyman, a number of themes have percolated to the top of our list for continued consideration:
- Confusion exists among agents/advisors about the nomenclature used to describe various combo products. What is the difference between combo, hybrid and linked? Is it time for the insurance industry to get together and create terminology accepted by all? Clarity should not be a rarity.
- Even more confusion exists about the differences between IRC Section 7702b long term care vs. 101g chronic illness benefits. What type of training should we create to address the differences, advantages, and disadvantages of these two types of solutions for long term care planning?
- Technology solutions offered by insurance companies get mixed reviews. Are we ready to examine what is working, and what is not, to make it easier for agents/advisors and consumers to access planning solutions?
- No consistent “COVID-19 message” pertaining to long term care planning has surfaced. Maybe it is too early, but it seems there are several obvious ones that agents/advisors could be utilizing.
- Agents/advisors continue to focus on the affluent market. However, the survey respondents indicated that expanding to the mid-market was of keen interest to them. What can carriers and distribution do to help create a larger playing field?
Stay tuned for more actionable intelligence from the WWWHW Survey.
References:
1. LIMRA—U.S. Individual Life Combination Products Annual Review 2019.
2. 2017 Thought Leadership Research—Lincoln Financial Group Versta Research.


















Forest Firestorms
Firestorms in the Pacific Northwest (Payroll deduction mandates) have blanketed our nation in smoke. Climate change (and COVID-19) reality have become the new buzz words for a clear understanding that we cannot go back. If there is an opportunity to change our future the reform must be profound and acknowledged as incremental and based on what we have learned from the conflagration. In recent conversations with knowledgeable cohorts in the struggle to at least bend the curve of long term care planning I have agreed to confirm my membership in the “Eternal Optimist Fraternal Association.” However there are some important caveats:
There is also a short list of those who have not failed :
Why we have continued to ignore the nose on our face has always amazed me. The model for what must be an obvious compromise between government mandates and private insurance solutions is certainly the intimate and successful marriage between Medicare and supplemental options to maintain personal responsibility, participate in the risk and reduce consumer cost to manageable levels. Guaranteeing an adequate level of program participation and therefore allowing affordable “gap” insurance, I would humbly submit, may have been the blueprint for reform all along.
Now there is smoke and there is fire. Evacuation orders to retreat to a new line of defense are drawn and pending. Please stay alert! Major structural changes are imminent; the landscape left after the fires burn out will not be the same. None of these smoldering fires or burning blazes are under control as this goes to press:
At this point, I am simply asking that you pay attention. The “conversations” are not necessarily bad ones but without your voices they could all go easily astray. Just so we are absolutely clear—the only voices I completely trust are those that read this column. These fires will leave a mark. I will do my best to keep you informed and forewarned.
Other than that I have no opinion on the subject.